
TL;DR:
- Regular self-examination using the ABCDE criteria helps identify suspicious skin lesions that warrant professional review. Photographs and noting changes over time are essential tools for monitoring skin health, especially in high-risk individuals. Prompt medical assessment and biopsy remain crucial for definitive diagnosis and effective treatment of potential skin cancers.
You notice something on your skin that wasn’t there before. Maybe a mole has changed shape, or a new spot has appeared that looks different from the rest. Knowing how to evaluate skin lesions at home is a skill that can genuinely save your life, yet most people either panic unnecessarily or, more dangerously, dismiss changes that warrant attention. This guide walks you through structured skin lesion assessment techniques, from setting up the right conditions for examination to understanding the red flags that mean you should see a specialist without delay.
Key takeaways
| Point | Details |
|---|---|
| Use the ABCDE criteria | Asymmetry, Border, Colour, Diameter, and Evolution form the foundation of any structured lesion check. |
| Photographs are your best tracking tool | Dated clinical photos allow you to compare lesions objectively over time, far better than memory alone. |
| AI apps have real limitations | AI diagnostic tools show lower accuracy in non-specialist settings and in darker skin tones, so treat results with caution. |
| Red flags demand prompt review | Bleeding, rapid growth, irregular borders, or colour changes require professional assessment, not a wait-and-see approach. |
| Biopsy gives the definitive answer | No self-assessment or imaging tool can replace histopathological confirmation for suspected skin cancer. |
How to evaluate skin lesions: understanding what you are looking at
The clinical term for examining and characterising a skin lesion is lesion assessment or dermatological evaluation. Before you can apply any assessment technique, you need a basic working knowledge of what different lesions look like and why some raise more concern than others.

Skin lesions broadly divide into two categories: primary lesions, which arise directly from skin changes, and secondary lesions, which result from progression or trauma to primary lesions. Within those groups, you will encounter a wide spectrum. Some are entirely benign, such as seborrhoeic keratoses (rough, waxy, stuck-on looking patches common in middle age), dermatofibromas (firm, brownish bumps that dimple inward when pinched), and ordinary melanocytic naevi, which are everyday moles.
Then there are the lesions worth watching closely. When differentiating skin lesions, these are the characteristics that raise suspicion:
- Colour variation within a single lesion: shades of brown, black, red, white, or blue within the same spot
- Irregular or poorly defined borders: edges that look ragged, notched, or that fade into surrounding skin
- Elevation or texture changes: a previously flat spot that now feels raised, crusted, or ulcerated
- Pearlescent or translucent appearance: a hallmark of basal cell carcinoma, particularly on the face
- Scaly, red patches that do not resolve: these can indicate squamous cell carcinoma or actinic keratosis, a precancerous lesion
Melanoma tends to look unlike your other moles. Basal cell carcinoma, the most common skin cancer type, often appears as a shiny or pearly nodule, sometimes with visible blood vessels. Squamous cell carcinoma typically presents as a firm, scaly lump or a persistent non-healing sore. Getting familiar with your own skin baseline, what is normal for you, is the single most valuable starting point.
Preparing for a thorough skin examination
Rushing a skin check in poor light with no record of what you find defeats the purpose entirely. Good preparation makes the difference between an examination that tells you something useful and one that leaves you guessing.
What you will need
| Tool | Purpose |
|---|---|
| Full-length mirror and hand mirror | Allows inspection of hard-to-see areas: back, scalp, behind ears |
| Smartphone with a good camera | Clinical and close-up photographs for documentation and sharing with clinicians |
| Bright, natural or daylight LED light | Accurate colour representation, critical for assessing skin tone changes |
| Ruler or millimetre gauge | Measuring lesion diameter objectively |
| Notebook or app for notes | Recording changes, dates, and observations systematically |
Before you begin, shower and allow your skin to dry fully. Remove nail polish if you are checking nails and fingers. Examine yourself in a warm, well-lit room where you feel relaxed. Photograph each lesion of concern from two distances: one wide shot showing the surrounding skin for context and one close-up. Dated clinical photographs allow you to compare lesions over time far more reliably than trying to remember what something looked like six months ago.
Some practical rules during preparation:
- Never squeeze, scratch, or attempt to remove any lesion before or during assessment. Trauma can alter its appearance and introduce infection.
- Use consistent lighting and position each time you photograph the same lesion so comparisons remain meaningful.
- Store photographs in a dedicated folder labelled with dates so you can share them quickly during a consultation or e-consultation.
Pro Tip: If you use a smartphone, enable the grid feature on your camera to keep photos consistently framed. Consistent angles make side-by-side comparisons far more reliable when you review images weeks or months later.
Assessing lesions systematically: the ABCDE method and beyond
Skin lesion assessment techniques are most effective when applied in a consistent, structured sequence. The ABCDE criteria remain the most widely taught framework for identifying potentially malignant lesions, particularly melanoma.
Here is how to work through them:
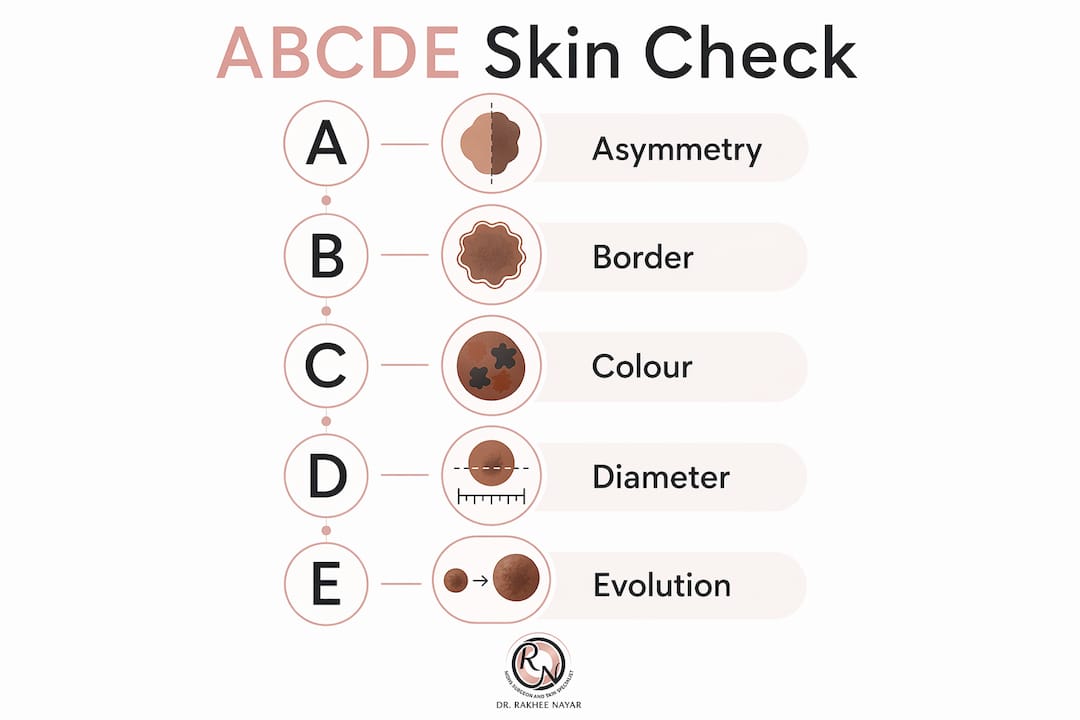
- Asymmetry: Draw an imaginary line through the centre of the lesion. If one half does not mirror the other, that is asymmetry. Benign moles are usually symmetrical.
- Border: Examine the edges. Irregular, ragged, notched, or blurred borders are concerning. A smooth, well-defined edge suggests a benign lesion.
- Colour: Look for variation within the lesion itself. A uniform tan or brown is generally reassuring. Multiple colours within the same spot warrant attention.
- Diameter: Lesions larger than 6 mm (roughly the diameter of a pencil eraser) warrant closer scrutiny, though smaller lesions can also be malignant and should not be ignored simply because they are small.
- Evolution: This is arguably the most important criterion. Any lesion that has changed in size, shape, colour, or texture over weeks to months deserves professional review. New symptoms such as itching, bleeding, or crusting also count as evolution.
Beyond ABCDE, the “Ugly Duckling” sign is a valuable addition to your toolkit. It refers to any lesion that simply looks different from your other spots, even if it does not tick the classic ABCDE boxes. Trust your instinct here.
Dermoscopy, the use of a specialised magnifying device with polarised light, is a significant step up from the naked eye. Dermoscopy increases diagnostic accuracy substantially: sensitivity for melanoma rises from 76% to 92% and for basal cell carcinoma from 79% to 93%. Consumer dermoscope attachments for smartphones exist, but their usefulness for self-examination is limited without training in dermoscopic pattern recognition.
As for AI-powered skin apps, be cautious. AI tools perform less well in community or smartphone settings compared with specialist environments, and accuracy drops further in Fitzpatrick IV to VI skin tones due to underrepresentation in training data. These apps can prompt you to seek advice, which is valuable, but they should never give you false reassurance that a lesion is safe.
Pro Tip: Rather than relying on a single assessment, examine the same lesion on two separate occasions, one week apart, before deciding whether to seek advice. Acute anxiety can affect your perception. A second look with fresh eyes, combined with your photographs, gives a calmer, more objective view.
Interpreting your findings and knowing when to act
Assessing skin abnormalities only has value if you know what to do with your findings. The purpose of self-evaluation is not to diagnose yourself. It is to decide whether and how urgently you need professional input.
Seek prompt professional review if you notice any of the following:
- A lesion that bleeds without injury, or that repeatedly crusts and fails to heal
- Any spot that has visibly changed in size, shape, or colour over four to eight weeks
- A new growth that looks distinctly different from your other moles or spots
- Itching, tingling, or tenderness within a lesion, especially if it is new
- Any pigmented lesion on the nail bed, sole of the foot, or mucous membranes
The comparison below illustrates the distinction between features that typically suggest a benign lesion and those that raise concern:
| Feature | Likely benign | Warrants review |
|---|---|---|
| Symmetry | Symmetrical | Asymmetrical |
| Borders | Smooth and defined | Irregular or poorly defined |
| Colour | Uniform tan or brown | Multiple colours or rapid colour change |
| Size | Stable, under 6 mm | Growing or over 6 mm |
| Surface | Smooth or uniformly rough | Ulcerated, bleeding, or crusted |
| Duration | Long-standing and unchanged | New or recently changed |
When you do consult a clinician, bring your dated photographs, notes on when you first noticed the lesion, and any history of sun exposure or previous skin cancers. A clinician will typically examine the lesion using dermoscopy as an intermediate step before deciding whether a biopsy is needed. Biopsy is required for definitive diagnosis, with excisional biopsy preferred for suspected melanoma. For lesions in cosmetically sensitive areas, a partial incisional biopsy targeting the most atypical region may be performed first.
Histopathological confirmation remains indispensable for melanoma, regardless of how confident any imaging or AI assessment appears. Teledermatology and digital second opinions can be helpful for initial triage, but they do not replace in-person clinical assessment for high-suspicion lesions.
Monitoring your skin safely between consultations
Consistent, structured self-monitoring is one of the most practical things you can do for your long-term skin health. This is especially true if you have a personal or family history of skin cancer, fair skin, a high mole count, or a history of significant sun exposure.
Practical habits to build into your routine:
- Self-examinations every three to four months are commonly recommended for higher-risk individuals, alongside an annual physician skin check.
- Apply broad-spectrum SPF 30 or higher daily, including during winter and on overcast days. UV exposure is cumulative and remains a primary driver of skin cancer risk.
- Consider mole mapping if you have numerous naevi or a personal history of skin cancer. Sequential digital dermoscopy and whole-body photography can reduce unnecessary biopsies while improving early detection in high-risk patients.
- Keep a simple skin diary. Photograph any new or changing lesion immediately and note the date. Review your photographs every three months alongside your next self-examination.
- Address anxiety proactively. Worry about skin lesions is completely understandable, but excessive anxiety that stops you from looking is counterproductive. Learning the criteria for identifying suspicious changes gives you agency rather than dread.
For ongoing skin care between appointments, explore evidence-based skin health practices that support prevention alongside regular monitoring.
My honest take on self-assessment and its limits
In my practice, I see a pattern. Patients arrive having monitored a lesion anxiously for months, waiting until it became impossible to ignore. The ABCDE rule is a genuinely useful framework, but I have seen melanomas that were relatively symmetrical and small, and I have seen alarming-looking seborrhoeic keratoses that were completely benign. The criteria are a guide, not a verdict.
What I have learnt from working with patients is that photographs are more useful than any app. Patients who bring a clear six-month photographic timeline give me an enormous diagnostic advantage. The evolution of a lesion over time tells a story that a single consultation appointment cannot fully capture.
I also see the damage caused by delay born of fear. A patient who avoids seeking advice because they are frightened of what they might hear will sometimes present with a cancer that required straightforward treatment six months earlier but now needs something more involved. Early review almost always means simpler treatment and better outcomes. If something concerns you, the answer is never to wait and hope.
Technology, including AI apps and consumer dermoscopes, supports informed vigilance. It is not a substitute for expert assessment. AI diagnostic accuracy in non-specialist settings remains imperfect, particularly across diverse skin tones. Use these tools to prompt action, not to avoid it.
— Rakhee
Expert care for suspicious skin lesions
If your self-assessment raises concern, the next step is a consultation with a specialist who combines diagnostic precision with the ability to manage whatever is found.

Rakhee Nayar – Mohs Surgeon and Skin Specialist offers expert evaluation and treatment for patients with suspicious or confirmed skin lesions, with a particular focus on skin cancers affecting the face and cosmetically sensitive areas. Miss Nayar’s dual training in plastic surgery and Mohs micrographic surgery means that diagnosis and treatment planning happen together, not in separate silos. Mohs micrographic surgery offers the highest cure rates for basal cell carcinoma and squamous cell carcinoma, removing cancerous tissue layer by layer while preserving as much healthy skin as possible. For patients who need it, reconstructive options are discussed from the outset. Private consultations and e-consultations are available for both UK-based and international patients. If a lesion has been worrying you, early expert review is always the right decision.
Common questions
What is the ABCDE rule for skin lesions?
The ABCDE rule stands for Asymmetry, Border, Colour, Diameter, and Evolution. It is a widely used framework to help identify features of potentially malignant skin lesions, particularly melanoma, during self-examination.
When should I see a doctor about a skin lesion?
See a doctor promptly if a lesion bleeds without cause, changes in size, shape, or colour over four to eight weeks, or looks clearly different from your other moles. New, persistent, or symptomatic spots also warrant professional review.
Can AI skin apps accurately diagnose skin lesions?
AI apps can prompt useful action but should not be relied upon for diagnosis. Pooled data shows AI sensitivity around 91%, but specificity is approximately 64%, with lower accuracy in non-specialist settings and in darker skin tones.
Is a biopsy always necessary to diagnose skin cancer?
Yes, biopsy provides the definitive diagnosis for skin cancer. Dermoscopy and clinical assessment guide the decision but cannot replace histopathological confirmation, particularly for suspected melanoma.
How often should I examine my skin at home?
Higher-risk individuals are advised to perform self-examinations every three to four months and to attend a physician skin check annually, though recommendations vary based on individual risk factors.

