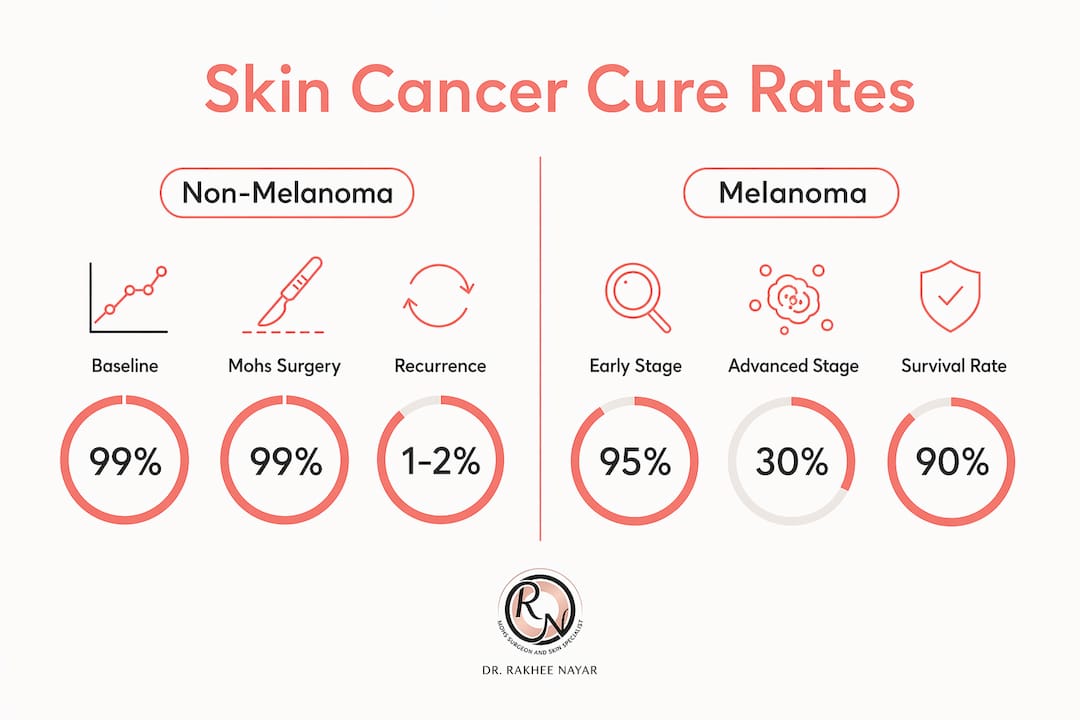
A high cure rate in skin cancer is defined as the probability that a given treatment removes all cancerous cells completely, with the patient remaining free of recurrence over a defined follow-up period, typically five to ten years. For non-melanoma skin cancers such as basal cell carcinoma (BCC) and squamous cell carcinoma (SCC), Mohs micrographic surgery achieves 5-year cure rates of 97 to 99%. These figures represent some of the highest treatment success rates in oncology. Melanoma, by contrast, is measured differently using relative survival statistics, with localised melanoma carrying a 5-year survival rate above 99% according to SEER data. Understanding what these numbers actually mean for your specific diagnosis is the most useful starting point.
What is a high cure rate in skin cancer, and how is it measured?
Cure rate and survival rate are related but distinct terms, and confusing them leads to unnecessary anxiety or, conversely, false reassurance. A cure rate in skin cancer refers specifically to the proportion of patients who achieve complete clearance of their cancer with no recurrence after treatment. Survival rate measures the proportion of patients alive at a set point in time, regardless of whether the cancer has returned or spread.
For non-melanoma skin cancers, researchers typically report clearance and recurrence-free survival over five to ten years. For melanoma, the standard metric is relative survival, which compares survival in cancer patients to the general population of the same age. This distinction matters because a patient with melanoma who is alive at five years may still carry residual disease, whereas a patient with BCC treated by Mohs surgery and recurrence-free at five years is, in practical terms, cured.
The phrase “high cure rate” has no universal threshold in oncology, but in clinical practice it generally refers to treatment success rates above 90%. BCC and SCC treated with Mohs surgery sit well above this threshold. Melanoma outcomes depend heavily on stage at diagnosis, ranging from excellent for localised disease to significantly reduced for distant metastatic disease.
Using a single cure rate figure for all skin cancers is clinically misleading. Specifying cancer type, stage, treatment method, and measurement timeframe is the only accurate way to interpret these statistics.
What factors influence how high the skin cancer cure rate is?
No single cure rate applies to every patient. Several medical and patient-specific factors determine where an individual’s prognosis sits within the published ranges.
Type of skin cancer is the primary determinant. BCC and SCC are non-melanoma skin cancers that rarely metastasise when caught early, making curative surgery achievable in the vast majority of cases. Melanoma carries a higher risk of spread and requires staging before prognosis can be estimated.
Stage at diagnosis has the greatest impact on outcome across all skin cancer types. Localised disease, confined to the skin, carries far better prospects than regional disease involving lymph nodes or distant metastatic disease. Recurrence rates and cure depend on tumour characteristics, patient health, and treatment timeliness, which is why early presentation to a specialist matters.
The following factors also influence cure rates significantly:
- Tumour size and depth. Larger or deeper tumours require wider surgical margins and carry higher recurrence risk.
- Tumour location. Cancers on the face, particularly around the nose, eyes, and ears, are classified as high-risk due to complex anatomy and the proximity of vital structures.
- Histological subtype. Morphoeic or infiltrative BCC, and poorly differentiated SCC, are more aggressive and harder to clear with standard excision.
- Previous treatment. Recurrent tumours, those that have been incompletely excised before, have lower cure rates than primary lesions treated for the first time.
- Patient immune status. Immunosuppressed patients, including organ transplant recipients, face significantly higher rates of SCC and reduced treatment success.
- Comorbidities. General health affects both surgical suitability and recovery, influencing the choice and timing of treatment.
Pro Tip: Ask your consultant to specify which risk category your tumour falls into. High-risk tumours have different appropriate-use criteria for Mohs surgery than low-risk lesions, and this classification directly affects the cure rate you can realistically expect.
How does Mohs micrographic surgery achieve high cure rates?
Mohs micrographic surgery is the treatment most consistently associated with the highest skin cancer cure rates for BCC and SCC. The procedure involves removing the visible tumour along with a thin margin of surrounding tissue, then immediately processing and examining 100% of the surgical margin under a microscope while the patient waits. If cancer cells are present at any margin, only that specific area is removed in the next stage. This continues until the margins are completely clear.

This approach contrasts sharply with conventional surgical excision, which examines only a small sample of the margin, typically 1 to 2% of the total tissue removed. The consequence is that standard excision can miss residual cancer at the margin, leading to recurrence.
The published data on this difference is substantial. For primary BCC, Mohs surgery cure rates are 98 to 99%, compared with 91 to 95% for conventional surgery. For recurrent BCC, Mohs achieves 94 to 98% cure rates versus 80 to 88% for conventional excision. The long-term recurrence figures are equally telling.
| Treatment | 10-year recurrence rate | Cure rate (primary BCC) |
|---|---|---|
| Mohs micrographic surgery | 4.4% | 98–99% |
| Conventional surgical excision | 12.2% | 91–95% |
| Mohs for recurrent BCC | Lower than excision | 94–98% |
| Conventional excision for recurrent BCC | Higher than Mohs | 80–88% |
Mohs surgery is the preferred method for high-risk facial skin cancers due to its tissue conservation and complete margin evaluation. This is particularly relevant for cancers near the eyes, nose, lips, and ears, where removing excess healthy tissue would cause significant functional or cosmetic harm. The dual benefit of maximum cure rate and minimum tissue loss makes it the treatment of choice in these anatomically sensitive locations.
Surgery remains the gold standard for localised skin cancer treatment. Radiotherapy, immunotherapy, and topical treatments exist as alternatives or adjuncts, but surgery delivers the highest cure rates for primary localised lesions. Advanced treatments such as cemiplimab show promise in advanced cutaneous SCC but do not replace surgery for primary disease.
Pro Tip: Mohs surgery is not appropriate for every skin cancer. Appropriate-use criteria developed by specialist bodies help identify which tumours benefit most. If you have a high-risk BCC or SCC on the face, ask specifically whether Mohs surgery is indicated for your case.
You can read more about Mohs vs standard excision to understand how the two approaches compare in practice.
What are the survival and cure rates for melanoma vs non-melanoma skin cancers?
Melanoma and non-melanoma skin cancers are measured by different outcome metrics, and comparing them directly without context produces misleading conclusions.
For non-melanoma skin cancers treated with curative intent, the focus is on clearance and recurrence-free survival. BCC and SCC treated appropriately achieve cure rates of 90 to 99%, depending on treatment method and tumour characteristics. These are among the most treatable cancers in medicine when caught at an early stage.
Melanoma is staged and reported differently. The 5-year relative survival rate for melanoma overall is approximately 95% based on SEER data from 2015 to 2021. However, this figure masks significant variation by stage. Localised melanoma carries a 5-year survival rate above 99%. Regional melanoma, where the cancer has spread to nearby lymph nodes, drops to 76%. Distant metastatic melanoma carries a 5-year survival rate of 35%. These statistics estimate the probability of treatment success across a population but do not predict individual outcomes.
| Cancer type | Stage | 5-year survival or cure rate |
|---|---|---|
| BCC (Mohs surgery) | Localised | 98–99% cure rate |
| SCC (Mohs surgery) | Localised | ~99% cure rate |
| Melanoma | Localised | >99% 5-year survival |
| Melanoma | Regional | 76% 5-year survival |
| Melanoma | Distant (metastatic) | 35% 5-year survival |
Younger and healthier patients have better melanoma survival outcomes regardless of stage, which reflects the role of immune function and overall fitness in treatment response. Advances in immunotherapy, including checkpoint inhibitors such as pembrolizumab and nivolumab, have substantially improved outcomes for advanced melanoma over the past decade, shifting what was once a poor prognosis disease into one with meaningful long-term survival for a proportion of patients.
The terminology difference between “cure rate” and “survival rate” is not merely academic. Non-melanoma skin cancer research uses clearance and recurrence-free survival because these cancers are almost always cured by surgery. Melanoma literature uses relative survival statistics because the disease can recur years after initial treatment, making the concept of cure more complex to define.
What practical steps can patients take to maximise treatment success?
The single most effective step a patient can take is early presentation. Skin cancers detected at a localised stage, before any spread to lymph nodes or distant sites, carry the highest cure rates across all types. Any new or changing lesion, particularly one that bleeds, crusts, fails to heal, or changes in colour or border, warrants prompt assessment by a specialist.
The following steps form a practical framework for maximising your skin cancer treatment success:
- Seek biopsy confirmation. A clinical diagnosis alone is insufficient. Histological confirmation by an experienced pathologist establishes the cancer type, subtype, and grade, all of which determine the most appropriate treatment. Biopsy review by experienced pathologists is fundamental to accurate treatment planning.
- Choose the right treatment for your tumour. Not all skin cancers require Mohs surgery, but high-risk BCC and SCC on the face, scalp, or other anatomically sensitive areas benefit most from it. Discuss with your consultant whether your tumour meets appropriate-use criteria.
- Select a surgeon with dual expertise. For facial skin cancers requiring both oncological clearance and reconstruction, a surgeon trained in both Mohs surgery and plastic surgery offers a significant advantage. Reconstruction planning should be considered before excision, not after.
- Attend all follow-up appointments. Recurrence, when it occurs, is most treatable when caught early. Follow-up schedules vary by cancer type and risk, but most specialists recommend annual skin checks for at least five years after treatment.
- Protect your skin consistently. Patients with a history of skin cancer have a higher risk of developing further lesions. Daily use of SPF 30 or higher, protective clothing, and avoidance of peak UV hours reduce this risk meaningfully.
Pro Tip: Before your consultation, write down the following questions: What type and subtype is my skin cancer? What stage is it? Is Mohs surgery appropriate for my case? What are the recurrence rates for the treatment you are recommending? What does follow-up look like? These questions will help you leave the consultation with a clear picture of your prognosis and plan.
For a detailed overview of what Mohs surgery involves and whether it is appropriate for your diagnosis, Miss Nayar’s patient resource covers the procedure, indications, and expected outcomes clearly.
Key takeaways
High cure rates in skin cancer are achievable for most patients with non-melanoma skin cancers when treatment is prompt, appropriate, and delivered by a specialist with the right expertise.
| Point | Details |
|---|---|
| Cure rate vs survival rate | Cure rate measures recurrence-free clearance; survival rate measures being alive at a set time point. |
| Mohs surgery leads on cure rates | Mohs achieves 98–99% cure for primary BCC and ~99% for SCC, versus 91–95% for conventional excision. |
| Melanoma outcomes vary by stage | Localised melanoma carries >99% 5-year survival; distant metastatic disease drops to 35%. |
| Early detection is the most effective intervention | Localised skin cancers treated promptly carry the highest cure rates across all types. |
| Tumour type and location determine treatment choice | High-risk or facial tumours benefit most from Mohs surgery due to complete margin evaluation. |
Why I think patients deserve clearer numbers, not just reassurance
By Miss Rakhee Nayar, Consultant Plastic Surgeon and Mohs Surgeon
One of the most common things I hear from patients at their first consultation is some version of: “My GP said it’s very treatable.” That is true for most skin cancers. But “very treatable” is not the same as understanding your specific cure rate, your recurrence risk, or why one treatment achieves better outcomes than another for your particular tumour.
What I have observed over years of treating BCC and SCC is that patients who understand the numbers make better decisions. They attend follow-up. They ask the right questions. They do not dismiss a new lesion two years later because they assume they are “cured.” The data on Mohs surgery is genuinely impressive, and I think patients deserve to hear it plainly rather than have it softened into vague reassurance.
The distinction between a 99% cure rate with Mohs and a 91 to 95% cure rate with standard excision may sound small in absolute terms. For a primary BCC on the nose treated once, that difference is meaningful. For a recurrent BCC where conventional excision drops to 80 to 88% success, the case for Mohs becomes clinically compelling, not just a preference.
I also want to be direct about what these statistics cannot do. They describe populations, not individuals. A patient with a morphoeic BCC on the inner canthus of the eye is not the same as a patient with a nodular BCC on the back. Individualised assessment, proper histological subtyping, and a clear reconstruction plan are what translate population statistics into the best possible outcome for a specific person.
The advances in melanoma treatment over the past decade have been genuinely significant. Immunotherapy has changed the outlook for advanced disease in ways that were not possible ten years ago. But for the non-melanoma skin cancers that make up the majority of cases I see, the most powerful tool remains precise surgical excision with complete margin control, delivered early.
— Miss Rakhee Nayar
Specialist Mohs surgery and skin cancer care with Miss Rakhee Nayar
If you have been diagnosed with BCC, SCC, or a suspicious lesion and want to understand your treatment options clearly, Miss Rakhee Nayar offers consultant-led assessments at her private clinic in North West England, with e-consultations available for patients across the UK and internationally.

Miss Nayar’s dual training in plastic surgery and Mohs micrographic surgery means that oncological clearance and facial reconstruction are planned together from the outset, not as separate afterthoughts. For patients with high-risk or facial skin cancers, this combined expertise directly supports the highest achievable cure rates. To explore whether Mohs surgery is appropriate for your diagnosis, or to review your treatment options, book a private consultation through mohssurgeon.co.uk.
This article is for informational purposes only and does not constitute medical advice. Please consult a GMC-registered specialist for assessment and treatment recommendations specific to your situation.
FAQ
What does a high cure rate in skin cancer actually mean?
A high cure rate means the treatment removes all cancer cells with no recurrence over a defined follow-up period, typically five to ten years. For BCC and SCC treated with Mohs surgery, this rate reaches 97 to 99%.
Is skin cancer always curable?
Most non-melanoma skin cancers are curable when treated promptly and appropriately. Melanoma is more variable; localised melanoma carries a 5-year survival rate above 99%, but distant metastatic melanoma drops to 35%, reflecting the importance of early diagnosis.
Why does Mohs surgery have a higher cure rate than standard excision?
Mohs surgery examines 100% of the surgical margin in real time, removing only tissue where cancer cells are confirmed present. Standard excision samples only a small fraction of the margin, which means residual cancer can be missed, leading to higher recurrence rates.
How do I know if Mohs surgery is right for my skin cancer?
Mohs surgery is most appropriate for high-risk BCC and SCC, particularly on the face, scalp, hands, and feet, or for recurrent tumours. Your consultant will assess tumour type, subtype, size, location, and previous treatment history to determine whether Mohs surgery meets appropriate-use criteria for your case.
What is the difference between cure rate and survival rate in skin cancer?
Cure rate refers to the proportion of patients who achieve complete clearance with no recurrence after treatment. Survival rate measures the proportion of patients alive at a specific time point, regardless of disease status. For melanoma, relative survival statistics are used because recurrence can occur years after initial treatment.