
TL;DR:
- Scars from Mohs surgery are biological and tend to improve significantly over 12 to 18 months.
- Risk factors like skin type, age, and wound tension influence scar severity and appearance.
- Early, targeted scar treatments such as steroids, silicone, and laser can improve outcomes.
Mohs micrographic surgery offers the highest cure rates for common skin cancers, yet one concern resurfaces for almost every patient once the wound is dressed and they head home: will this scar badly? The worry is understandable. You have had tissue removed from your face or another visible area, and the early result can look alarming. What many patients do not realise is that layer-by-layer excision is designed to conserve as much healthy tissue as possible, and that what you see in week one is rarely what you will see in year two. This article explains the biology of post-Mohs scarring, the full healing timeline, the risk factors worth knowing, and the treatments available when scars need extra help.
Key Takeaways
| Point | Details |
|---|---|
| Scar formation is normal | All Mohs surgery patients develop scars, but most fade with time and proper care. |
| Scar appearance improves | Scars can look raised or red early on, yet generally flatten and blend in after 12-18 months. |
| Prevention and treatment work | Proactive scar care and modern therapies help minimise and improve even difficult scars. |
| Patient factors matter | Genetics, skin type, and surgical site influence scar severity—individualised care is key. |
| Expert help is available | Specialist follow-up and advanced reconstructive options offer the best outcomes for complex cases. |
Why does scarring occur after Mohs surgery?
Every surgical wound creates a scar. That is not a failing of the surgeon or the technique; it is biology. When skin is cut and tissue is removed, the body launches a repair response that lays down collagen to close the gap. That new collagen never organises itself exactly as the original skin did, which is why a scar looks and feels different from surrounding tissue, at least initially.
What makes Mohs special is the degree to which it limits that damage. Because cancer clearance prioritises minimal tissue loss, the surgeon removes only the cancer and a very thin margin of surrounding skin, checking each layer under the microscope before deciding whether to go deeper. Traditional wide-local excision, by contrast, removes a larger safety margin without that real-time confirmation, meaning more healthy skin goes unnecessarily. Less removed tissue means a smaller wound, which typically means a smaller scar.
The size and shape of the final scar also depends on how the wound is closed after the cancer is out. Your surgeon will choose the reconstruction method that suits the defect:
- Primary closure (stitching the wound edges directly together): produces a fine linear scar, works when there is enough surrounding tissue laxity.
- Local flap: nearby skin is rotated or advanced to cover the defect, offering excellent colour and texture matching, particularly on the face.
- Skin graft: skin taken from a donor site (often behind the ear or inner arm) is used to cover larger or complex defects.
- Secondary intention: the wound is left to heal naturally, often chosen for specific facial sites such as the inner corner of the eye where the result can be surprisingly good.
Each method has aesthetic trade-offs, and the goal is always restoring function and confidence alongside cancer clearance. Understanding which closure you had helps you interpret what your healing scar should look like over time.
Pro Tip: Ask your surgeon which closure method was used and request a rough sketch of where your incision lines lie. Knowing your scar’s anticipated shape makes it far easier to track progress during recovery.
How do scars heal and change after Mohs surgery?
Knowing that a scar will improve is one thing. Understanding why and when makes those first anxious weeks considerably easier to navigate. Wound healing after Mohs surgery follows four overlapping phases, each with a distinct biological purpose.
The four phases of healing
- Haemostasis (minutes to hours): Blood vessels constrict, platelets clump together, and a clot forms. This is the body’s emergency repair response. Your wound may weep slightly during this phase, which is entirely normal.
- Inflammation (days 1 to 7): The area becomes red, warm, and swollen as white blood cells clear debris and bacteria. This can look alarming but serves a vital protective purpose. Confusing normal inflammation with infection is one of the most common mistakes patients make.
- Proliferation (weeks 1 to 4): Fibroblast cells produce new collagen rapidly. The scar may feel firm, itchy, or raised during this phase. Many patients find this the most visually uncomfortable stage because the scar can look more prominent than immediately after surgery.
- Remodelling and maturation (months 1 to 18): The collagen fibres reorganise into a stronger, more ordered structure. The scar softens, flattens, and fades. The final colour and texture are not visible until this phase completes, which can take up to 18 months.
What to expect at each stage
| Time after surgery | Typical scar appearance | What is happening |
|---|---|---|
| Week 1 | Red, swollen, possibly crusted | Inflammation, initial collagen laid |
| Weeks 2 to 4 | Raised, firm, potentially itchy | Rapid collagen production |
| Months 2 to 6 | Pinkish, still slightly raised | Collagen remodelling begins |
| Months 6 to 12 | Flatter, colour fading towards skin tone | Maturation continues |
| Months 12 to 18 | Near-flat, pale or skin-coloured | Mature scar, close to final appearance |
“The single biggest mistake is judging a post-surgical scar at six weeks. The scar you see at six weeks is not the scar you will have at eighteen months.”
Following skin health tips for recovery during all four phases gives your body the best chance to produce a well-matured result. Protecting the scar from sun exposure, keeping it moisturised, and avoiding smoking are particularly influential on final outcomes.

Pro Tip: Apply a broad-spectrum SPF 50 sunscreen to the scar every morning from week three onwards. UV exposure can permanently darken immature scars through post-inflammatory hyperpigmentation, and this discolouration is far harder to treat than the underlying scar itself. Guidance on minimising scarring after skin cancer removal goes into further detail on aftercare products and routines.
What factors influence the severity or appearance of scars?
Most Mohs scars settle well within the first year. But some patients develop thicker, more prominent, or persistent scarring. Understanding the risk factors helps you anticipate your own trajectory and seek early intervention if needed.
Types of problematic scars
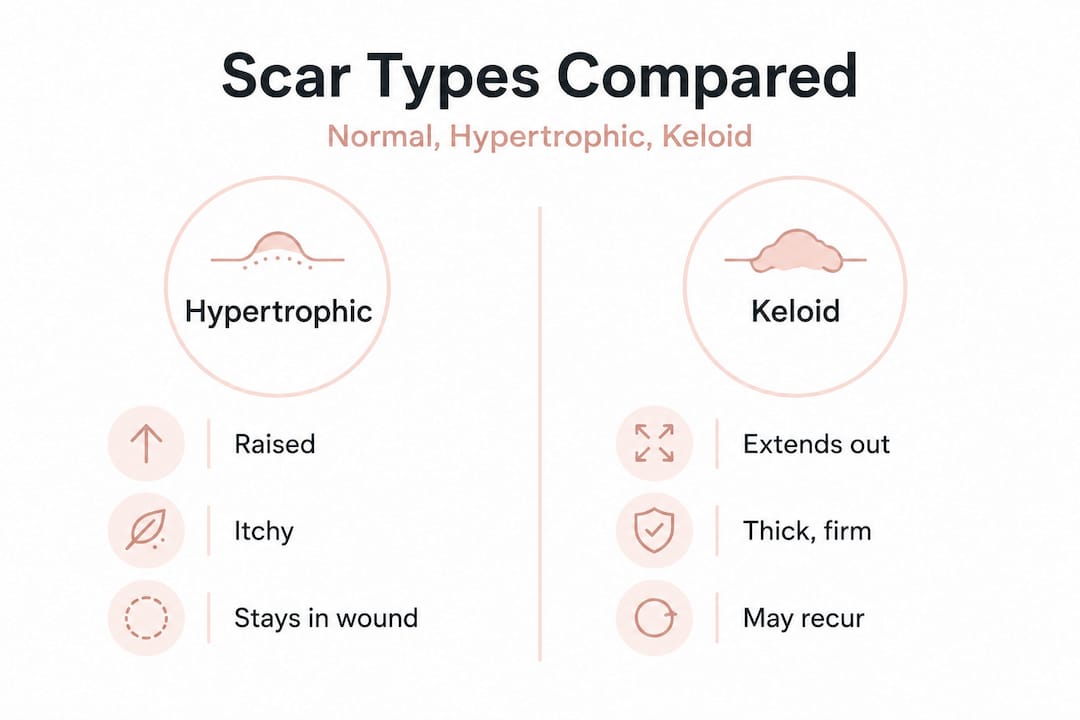
Not all difficult scars behave the same way. The two main categories are hypertrophic scars and keloids.
Hypertrophic scars are raised and firm but stay within the original wound boundary. They often itch and may feel tight. Importantly, they frequently regress on their own over 12 to 24 months and generally respond well to treatment. Many patients mistake them for keloids when they first appear, but the prognosis is considerably more favourable.
Keloids are a different matter. They grow beyond the original wound edges, sometimes extending significantly into surrounding skin. They are associated with higher risk in darker skin types, specifically Fitzpatrick phototypes IV to VI, as well as in younger patients, those with a family history of keloid formation, and those with hypertension. Keloids rarely regress without treatment and carry a high recurrence rate even after excision.
Key risk factors at a glance
- Skin type: Fitzpatrick IV to VI skin carries a meaningfully higher risk of keloid formation. This is an intrinsic genetic factor, not something lifestyle changes can easily overcome.
- Age: Younger patients, particularly those under 30, scar more aggressively because their collagen production is more vigorous.
- Anatomic location: The central chest, shoulders, and upper back are high-tension zones where wounds are constantly being pulled apart as you breathe and move. Facial wounds, despite their visibility, often heal very well because facial skin is rich in blood supply.
- Genetics: A family history of keloid or hypertrophic scarring is a significant predictor, even before the operation.
- Wound tension: Poorly placed or closed wounds that sit under tension heal less cleanly. This is why surgical planning for natural-looking Mohs reconstructions is critical from the outset.
- Medical history: Diabetes, immunosuppression, or conditions requiring anticoagulants can slow healing and alter scar quality.
Comparing scar types
| Feature | Normal scar | Hypertrophic scar | Keloid |
|---|---|---|---|
| Boundary | Within wound | Within wound | Extends beyond wound |
| Colour | Fades to skin tone | Red, persists longer | Pink to dark red |
| Texture | Flat over time | Raised, firm | Hard, nodular |
| Spontaneous regression | Yes | Often | Rarely |
| Treatment response | Minimal needed | Good | Variable, high recurrence |
Discussing your personal risk profile before or shortly after surgery allows your care team to personalise your follow-up. Your reconstruction choices may even be influenced by known risk factors identified at your initial consultation.
How are problematic scars after Mohs managed or improved?
Difficult scars are not a dead end. A wide range of evidence-based treatments exists, and early referral to a specialist generally produces far better results than watchful waiting.
First-line treatments
- Intralesional corticosteroid injections (triamcinolone): The most commonly used first-line treatment for hypertrophic scars and keloids. Injections are given directly into the scar at intervals of four to six weeks. They reduce collagen overproduction and flatten the tissue. Most patients need a course of three to six sessions.
- Silicone gel sheeting or gel: Worn over the scar for at least 12 hours per day, silicone creates an occlusive environment that softens and flattens raised scars. It works best when started early and used consistently for at least three months.
- Pressure therapy: Particularly useful for larger grafted areas, pressure garments reduce blood flow to the scar and limit excessive collagen deposition.
Advanced and combination treatments
- Laser therapy: Pulsed-dye laser targets the red pigmentation and blood vessels feeding hypertrophic scars. Fractional CO2 or erbium lasers can resurface the scar surface and improve texture. Laser works best on scars that are already relatively flat or have been partially treated with steroids.
- Microneedling: Creates controlled micro-injuries that stimulate regulated collagen remodelling. Evidence suggests that combination therapies are superior to single modalities, and microneedling is frequently paired with steroid infusion or platelet-rich plasma.
- 5-fluorouracil (5-FU) injections: An adjunct to steroid injections, particularly for keloids. 5-FU disrupts fibroblast activity and reduces collagen synthesis. It is often used when steroid injections alone are insufficient.
- Surgical revision: For scars with poor orientation or excessive tension, procedures such as Z-plasty (which repositions the scar along natural tension lines) can dramatically improve appearance.
- Radiotherapy: Reserved primarily for keloids following surgical excision, post-operative radiotherapy reduces recurrence rates substantially. It is not routinely used for hypertrophic scars.
Pro Tip: Do not wait until a scar has fully matured before seeking help for a problematic result. Intervening in the proliferative phase (weeks two to twelve) is significantly more effective than attempting to remodel a fully mature, established scar. If your scar is thickening rapidly or causing discomfort, request an early review. Detailed guidance on minimising visible scarring covers what to look out for and when to act.
Our expert take: why scar anxiety is often misplaced
There is an uncomfortable truth about scar anxiety after Mohs surgery: most patients arrive expecting the worst, and most leave with results far better than they anticipated. Yet the gap between fear and outcome persists, largely because patients are judging a six-week wound as if it represents the final result.
No surgery, however skilled, leaves skin completely unchanged. That needs to be stated plainly. Anyone who promises scarless results is offering something that biology does not support. What Mohs does offer is tissue conservation, precision, and access to reconstructive options that give the scar its best possible start. The biology of abnormal scarring involves dysregulation of transforming growth factor beta (TGF-β), a signalling molecule that drives excessive collagen production in susceptible individuals. This is not something visible at the time of surgery, which is why identifying high-risk patients before or immediately after the procedure matters enormously.
What we have observed consistently is that patients who are given clear, realistic expectations before surgery experience far less distress during recovery. They understand that redness is normal, that itching means collagen is being laid down, and that the final result is at least 12 months away. Contrast this with patients who expect an invisible scar within weeks: their entirely normal healing trajectory feels like failure. Access to expert insights on surgical aesthetics alongside your Mohs procedure can make a measurable difference to how you experience and interpret your recovery.
Where to get expert advice and care for Mohs scars
Recovering from skin cancer surgery involves far more than clearing the cancer itself. The weeks and months that follow bring their own questions, anxieties, and decisions. For many patients, having access to a specialist who understands both the oncological and the aesthetic dimensions of their care makes a profound difference.

At mohssurgeon.co.uk, Miss Rakhee Nayar brings unique dual training in both Mohs surgery and plastic surgery, meaning that reconstruction is considered from the moment of your initial diagnosis rather than as an afterthought. Whether you are concerned about a thickening scar, considering revision options, or simply want to understand what your recovery should look like, tailored support is available. Explore the detailed guidance on minimising scars after Mohs or learn more about facial reconstruction options to understand what is possible when the best surgical and reconstructive expertise are combined under one specialist’s care.
Frequently asked questions
How long does it take for Mohs scars to fully heal?
Scars mature over 12 to 18 months, becoming progressively flatter and less pigmented as the remodelling phase continues. The appearance at six weeks is not representative of the final result.
What makes some people prone to thicker or raised scars after surgery?
Higher risk of hypertrophic or keloid scarring is associated with darker skin phototypes, younger age, high-tension anatomical sites, family history of keloid formation, and hypertension. Identifying these factors early allows preventive strategies to be put in place.
Can scars after Mohs be made less visible?
Yes. Early wound care, consistent silicone gel use, intralesional steroids and laser therapy can all meaningfully improve scar appearance. Combination approaches generally outperform single treatments.
Will facial scars from Mohs surgery always be obvious?
Most facial scars fade significantly within 12 to 18 months, often becoming very difficult to detect with the naked eye. Individual outcomes vary based on skin type, location, and aftercare quality, but a good result is far more common than patients initially expect.


