
TL;DR:
- Mohs surgery offers a 99% cure rate and maximizes tissue preservation, especially on the face.
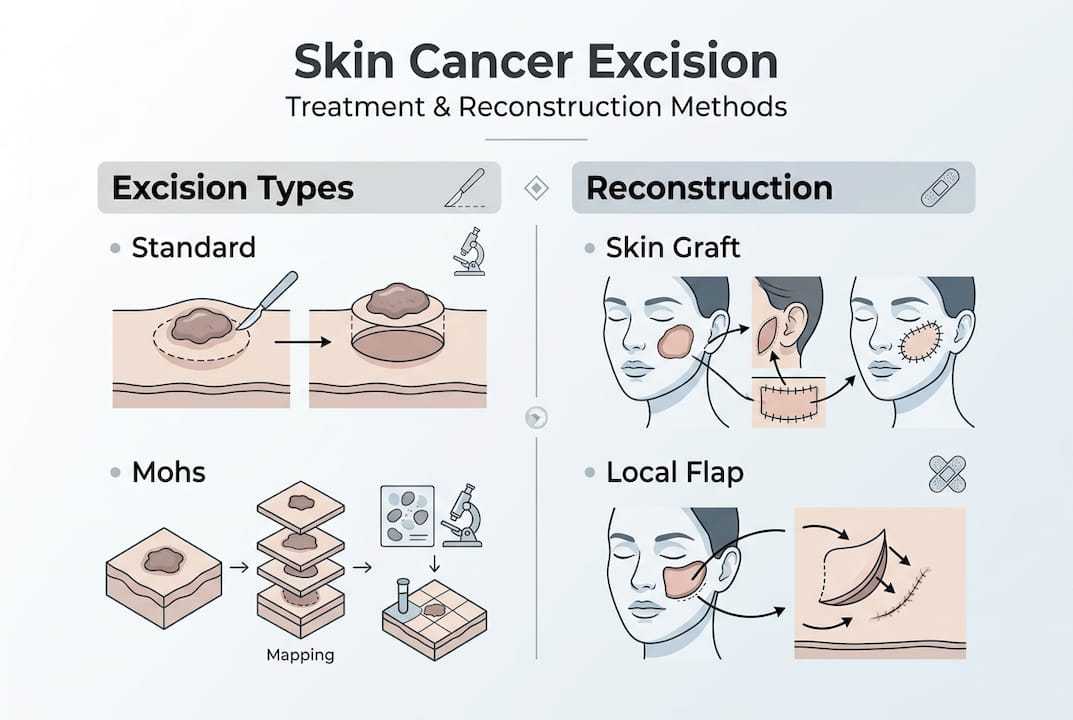
- Standard excision involves removing the tumor with a margin and analyzing tissue later, with slightly lower cure rates.
- Facial reconstruction methods include skin grafts and flaps, prioritized for function and cosmetic outcomes.
Mohs micrographic surgery achieves a cure rate of up to 99% for skin cancers such as basal cell carcinoma, yet many patients arrive at their first consultation believing all skin cancer surgery is essentially the same. It is not. The choice between standard surgical excision and Mohs surgery can significantly affect your cure rate, how much healthy tissue is preserved, and the final appearance of your face. This guide explains what surgical excision involves, how it compares to Mohs surgery, what facial reconstruction entails, and when one approach is clearly preferable to the other.
Guide to Skin Cancer Excision, Mohs Surgery & Reconstruction
- What is surgical excision?
- Mohs micrographic surgery versus traditional excision
- Facial reconstruction after surgical excision
- When is Mohs surgery recommended over standard excision?
- Our perspective: Making surgical choices for skin cancer on the face
- Explore expert surgical excision and facial reconstruction solutions
- Frequently asked questions
Key Takeaways
| Point | Details |
|---|---|
| Surgical excision basics | It removes skin cancer and surrounding tissue under local anaesthetic, tailored to tumour risk. |
| Mohs surgery advantages | Mohs procedure offers up to a 99% cure rate and minimises tissue loss for facial cancers. |
| Reconstruction options | Expert reconstruction uses skin grafts or flaps, focusing on both appearance and function. |
| When Mohs is needed | Mohs is recommended for high-risk, recurrent, or cosmetically sensitive facial tumours. |
What is surgical excision?
Surgical excision is the most widely used technique for removing skin cancer in the UK. In straightforward terms, it means cutting out the visible tumour along with a surrounding border of apparently healthy skin, known as the surgical margin. The aim is to ensure no cancer cells are left behind at the edges of the removed tissue.
The procedure is typically performed as a day case under local anaesthetic, meaning you remain awake but the treated area is completely numb. As BAPRAS confirms, surgical excision involves removing the visible tumour and a margin of healthy skin under local anaesthetic, making it accessible and well-tolerated for most patients.
Here is what the process generally involves:
- Assessment and marking: The surgeon maps the tumour boundaries and marks the planned excision margin on the skin.
- Local anaesthetic injection: The area is numbed before any incision is made.
- Excision: The tumour and surrounding margin are cut away in a single elliptical or circular piece.
- Specimen sent to pathology: The removed tissue is sent to a laboratory, where a pathologist checks whether the margins are clear of cancer cells.
- Wound closure: The wound is closed using sutures, and reconstruction is planned based on defect size and location.
The width of the margin taken depends on the tumour type, size, and risk level. Low-risk basal cell carcinomas may need only a 3 to 4 mm margin, while higher-risk or larger tumours may require a wider excision. Understanding your tumour’s risk profile is essential before choosing a surgical approach. You can read more about this in our high-risk skin cancer guide.
Important: Standard excision sends tissue to an external laboratory, which means results can take several days. If margins are not clear, a second operation may be needed.
For patients with basal cell carcinoma on the face, it is worth understanding how the tumour presents before surgery. Our guide on identifying basal cell carcinoma covers the key warning signs. The BAPRAS skin cancer overview also provides a reliable starting point for understanding your diagnosis within a UK clinical context.
Mohs micrographic surgery versus traditional excision
Mohs micrographic surgery is a specialised technique that differs fundamentally from standard excision in how tissue is removed and examined. Rather than taking a single block of tissue with a fixed margin, Mohs surgery removes the cancer in thin, sequential layers. Each layer is immediately processed and examined under a microscope, with 100% of the surgical margin checked in real time.
This matters enormously. Standard excision typically analyses only a small sample of the margin, which means some cancerous tissue can be missed. Mohs, by contrast, examines 100% of margins and achieves a cure rate of up to 99%, while removing the smallest possible amount of healthy tissue.
| Feature | Standard excision | Mohs surgery |
|---|---|---|
| Margin analysis | Partial sample | 100% of margin |
| Cure rate | Around 90 to 95% | Up to 99% |
| Recurrence rate | 5 to 10% | 1 to 3% |
| Tissue conservation | Moderate | Maximum |
| Results available | Days later | Same day |
| Best suited for | Low-risk, non-facial sites | Facial, high-risk, recurrent |
The recurrence rate difference is clinically significant. A recurrence rate of 1 to 3% with Mohs compared to 5 to 10% with standard excision means that for facial cancers, where re-excision carries real cosmetic and functional consequences, the choice of technique is not trivial.
Statistic to note: Mohs surgery’s recurrence rate of 1 to 3% is roughly three to five times lower than that of standard excision, making it the preferred choice for high-risk facial sites.
Pro Tip: If you have been told your skin cancer is on or near the nose, eyelids, ears, or lips, ask your surgeon specifically whether Mohs surgery is appropriate. These are high-risk anatomical sites where tissue conservation is critical.
There are also common misconceptions worth addressing. Many patients assume Mohs surgery is far more invasive or painful than standard excision. In practice, both procedures use local anaesthetic and are performed as day cases. You can explore the evidence behind these assumptions in our article on Mohs surgery myths vs facts, and get a full procedural overview in our guide on what is Mohs micrographic surgery.
Facial reconstruction after surgical excision
Removing a skin cancer from the face inevitably leaves a defect, and how that defect is repaired is just as important as the excision itself. Reconstruction is not simply about aesthetics, though appearance matters greatly. It is also about restoring function: protecting the eye, preserving the lip seal, maintaining the nasal airway.

The two primary methods for repairing facial defects are skin grafts and flaps. As BAPRAS confirms, skin grafts and flaps are the primary methods for reconstruction after excision, with cosmetic outcome as a key priority.
| Technique | What it involves | Best used for |
|---|---|---|
| Split-thickness graft | Thin layer of skin from donor site | Larger defects, less cosmetically sensitive areas |
| Full-thickness graft | Full skin layer from donor site | Smaller facial defects, better colour match |
| Local flap | Adjacent tissue rotated into defect | Most facial reconstructions |
| Regional flap | Tissue from nearby area with own blood supply | Larger or complex defects |
Flaps are generally preferred for facial reconstruction because, as NCBI research shows, facial flaps match skin lines and colour for optimal reconstruction, producing far more natural-looking results than grafts in most cases.
Key considerations your surgeon will weigh include:
- Defect size and depth: Larger or deeper wounds require more complex reconstruction.
- Location on the face: The nose, eyelids, and lips each have specific functional requirements.
- Skin laxity: Older patients often have more tissue available for local flaps.
- Timing: Immediate reconstruction is usually preferred, but delayed reconstruction may be chosen when tumour clearance is uncertain.
Pro Tip: Ask your surgeon whether they have specific training in both oncological excision and reconstructive surgery. Having both skills in one specialist significantly reduces the risk of functional or cosmetic compromise.
You can explore the full range of options in our detailed guide on facial reconstruction surgery, understand the principles behind what is facial reconstruction, and read about reconstruction after Mohs surgery specifically. For squamous cell carcinoma cases, our page on SCC diagnosis and facial reconstruction provides additional context.
When is Mohs surgery recommended over standard excision?
Not every skin cancer requires Mohs surgery, but for certain cases it is unambiguously the better option. Understanding when Mohs is clinically indicated helps you ask the right questions and advocate for the most appropriate care.
UK clinical consensus supports Mohs surgery in the following situations:
- High-risk anatomical sites: Tumours on the nose, eyelids, ears, lips, and temples, where tissue conservation directly affects function and appearance.
- Aggressive tumour subtypes: Morphoeic, infiltrative, or micronodular basal cell carcinomas, which have poorly defined borders and a higher likelihood of subclinical spread.
- Recurrent tumours: Cancers that have returned after previous treatment, where scar tissue makes margin assessment more difficult.
- Ill-defined borders: Tumours where the edges are not clearly visible clinically, increasing the risk of incomplete excision.
- Previous incomplete excision: When a prior operation did not achieve clear margins, Mohs provides the most reliable path to complete removal.
As Skin Health Info confirms, Mohs is preferred for high-risk, recurrent, or cosmetically sensitive areas, and for ill-defined tumours or previous incomplete excision.
UK expert consensus: UK specialists favour Mohs for facial cases specifically because it spares the maximum amount of healthy tissue while minimising recurrence risk, two goals that are often in direct tension with standard excision.
The decision should ideally involve a multidisciplinary team (MDT), particularly for complex or recurrent cases. An MDT brings together dermatologists, surgeons, oncologists, and pathologists to ensure the treatment plan is tailored to your specific tumour, not just its category. Our guide on preparing for Mohs surgery walks you through what to expect, and our Mohs surgery UK page provides a full service overview.
Our perspective: Making surgical choices for skin cancer on the face
Guidelines are invaluable, but they do not make decisions. Patients do, ideally with a surgeon who understands both the oncological and reconstructive dimensions of their case.
One assumption we encounter regularly is that standard excision is always sufficient if the tumour appears small or well-defined. This is not always true. Skin cancers on the face, particularly basal cell carcinomas with certain growth patterns, can extend well beyond their visible borders. A tumour that looks contained may have subclinical fingers of cancer reaching into surrounding tissue.
This is precisely why the choice of surgical technique matters as much as the decision to operate. Choosing Mohs surgery for a recurrent or morphoeic tumour on the nose is not overcautious. It is clinically sound. Equally, not every small, low-risk lesion on the trunk requires Mohs. Appropriate matching of technique to tumour is the mark of genuinely expert care.
We also believe strongly in MDT input for any case that sits outside the straightforward category. If there is any doubt about tumour subtype, margin definition, or reconstruction complexity, a second specialist opinion can be the difference between one operation and three. Our high-risk treatment guide outlines what that level of care looks like in practice.
Explore expert surgical excision and facial reconstruction solutions
If you have been diagnosed with a facial skin cancer or are seeking a second opinion on a previous excision, understanding your surgical options is the first step. Choosing the right technique, whether standard excision or Mohs surgery, and pairing it with skilled facial reconstruction can make a significant difference to both your cure rate and your quality of life.

Miss Rakhee Nayar holds dual training in plastic surgery and Mohs micrographic surgery, a combination that is rare in the UK and directly relevant to complex facial cases. Whether you are considering explore Mohs micrographic surgery for the first time or want to understand your reconstruction options, our facial reconstruction services page outlines what expert care looks like. Private consultations and e-consultations are available for UK and international patients.
Frequently asked questions
What is the main goal of surgical excision in skin cancer treatment?
The main goal is to remove all visible tumour and achieve clear surgical margins to minimise the risk of recurrence. Wide local excision is designed specifically to ensure no cancer cells remain at the wound edges.
How do Mohs surgery and standard excision differ?
Mohs surgery analyses 100% of excised margins microscopically in real time, offering higher cure rates and superior tissue conservation, particularly for facial cancers where preserving healthy skin is critical.
What methods are used for facial reconstruction after excision?
Skin grafts and flaps are the most common techniques, with the choice depending on defect size, location, and cosmetic requirements. Facial defects are repaired using whichever method best restores both function and appearance.
When is Mohs surgery especially recommended for UK patients?
Mohs is best for high-risk facial sites, recurrent tumours, aggressive subtypes such as morphoeic basal cell carcinoma, or cases where tumour borders are ill-defined or a previous excision was incomplete.

