
TL;DR:
- Skin cancer staging determines how far the tumor has spread, guiding treatment and prognosis. It involves biopsy, lymph node assessment, and imaging to classify the disease from stage 0 to IV. Accurate staging, specific to cancer type, is essential for appropriate management and better outcomes.
Receiving a skin cancer diagnosis brings a flood of questions, and one of the first things most people want to know is what stage they are at. Understanding how is skin cancer staged matters enormously because staging drives treatment decisions and shapes your prognosis from the very start. Yet staging is widely misunderstood. Many people assume that a larger or darker lesion automatically means a more advanced stage. The reality is far more nuanced, and knowing why can help you engage more confidently with your medical team and make sense of every step ahead.
Key takeaways
| Point | Details |
|---|---|
| Staging guides treatment | The stage assigned to your skin cancer directly determines whether you need surgery alone or a combination of therapies. |
| TNM classification is the framework | Tumour size, lymph node involvement, and distant spread are the three pillars used to classify skin cancer stage. |
| Biopsy is non-negotiable | Microscopic examination of tissue, not visual inspection alone, is what accurately assigns a stage. |
| Early detection changes outcomes | Shallow, early-stage melanomas carry a nearly 100% cure rate after surgery. |
| Staging varies by cancer type | Melanoma, squamous cell carcinoma, and Merkel cell carcinoma each use distinct staging criteria and carry different prognostic implications. |
How is skin cancer staged: the basics
Staging is the process doctors use to describe how far a cancer has grown and whether it has spread beyond its original site. In practical terms, it answers three questions: How deep or large is the primary tumour? Have cancer cells reached nearby lymph nodes? Has the cancer spread to distant organs?
The answers to these questions place a patient into a stage group, typically from 0 to IV, where stage 0 represents cancer cells confined to the outermost layer of skin and stage IV represents cancer that has spread to distant sites. This skin cancer classification system is not a single universal formula. Different skin cancers use different criteria.
Here is why the distinction between cancer types matters for staging:
- Melanoma is staged using detailed pathologic factors including tumour thickness, ulceration, and lymph node status, making the TNM classification particularly granular.
- Basal cell carcinoma (BCC) rarely metastasises and is often treated without formal full staging, although the AJCC 8th edition does provide staging criteria for high-risk cases.
- Squamous cell carcinoma (SCC) uses TNM staging that accounts for perineural invasion, bone involvement, and nodal spread.
- Merkel cell carcinoma, a rare but aggressive cancer, relies heavily on staging to guide treatment intensity. Staging shapes the entire care pathway for this type.
Understanding what type of skin cancer you have is the starting point for understanding your own staging process. You can read more about the differences between these diagnoses in this overview of skin cancer types and treatments.
The TNM system: what each letter means
The TNM framework is the backbone of how to determine skin cancer stage for most skin cancers. Each letter captures a specific dimension of the cancer’s behaviour.
T: the tumour itself
For melanoma, the T category is defined primarily by Breslow depth, which is the measured thickness of the tumour from the skin surface down to its deepest point, and by whether the tumour surface is ulcerated. Tumours of similar visible size can belong to entirely different T categories based solely on these microscopic characteristics. A 6mm melanoma with ulceration is staged more seriously than a 6mm melanoma without it.

For non-melanoma skin cancers, the T category uses tumour diameter along with features such as perineural invasion, depth of invasion into bone or muscle, and location on specific high-risk anatomical sites.
N: lymph node involvement
The N category captures whether cancer cells have reached the regional lymph nodes. What makes this genuinely complex is that cancer cells can spread to lymph nodes long before those nodes feel enlarged on physical examination. This is precisely why sentinel lymph node biopsy (SLNB) matters so much. SLNB detects microscopic nodal spread that imaging simply cannot reveal, making it the key step between a localised and a regional disease classification.
M: distant metastasis
The M category records whether cancer has spread to distant organs such as the lungs, liver, brain, or bone. An M1 designation moves a patient directly to stage IV regardless of the T or N values.
| TNM component | What it measures | Key tools used |
|---|---|---|
| T (Tumour) | Depth, size, ulceration | Biopsy, pathology report |
| N (Nodes) | Lymph node involvement | Sentinel node biopsy, imaging |
| M (Metastasis) | Distant organ spread | CT, PET, MRI scans |
Pro Tip: Ask your pathologist or consultant specifically for your Breslow depth and ulceration status if you have melanoma. These two numbers carry enormous weight in your staging, and understanding them helps you ask better questions about your treatment options.
How biopsy and imaging tests determine stage
Staging is never done by eye. Biopsy pathology is the foundation on which every staging decision rests. Here is the typical diagnostic sequence used to gather the information needed for accurate staging:
-
Excisional or punch biopsy removes all or part of the suspicious lesion so a pathologist can examine the tissue under a microscope. This confirms the diagnosis and provides the first pathologic data, including Breslow depth and ulceration status for melanoma.
-
Sentinel lymph node biopsy is recommended for melanomas with a Breslow depth above 0.8mm, or for thinner melanomas with ulceration. A small amount of tracer dye identifies which lymph node is the first likely destination for spreading cells. That node is removed and examined microscopically. SLNB markedly improves staging accuracy and influences stage grouping even when no clinical lymph node enlargement is present.
-
Imaging studies such as CT, PET-CT, or MRI are selected based on tumour thickness and risk factors rather than applied universally. Staging studies are tailored to the individual patient’s risk profile, so not everyone with skin cancer will need a full body scan.
-
Genetic and molecular testing can be performed on the tumour tissue in certain melanoma cases. Mutation testing may guide treatment decisions particularly when systemic therapies such as targeted agents or immunotherapy are being considered for advanced disease.
Understanding this sequence helps demystify what can feel like an overwhelming series of appointments. Each test answers a specific staging question, and together they build the complete picture.
Skin cancer stages explained: from 0 to IV
Once the TNM components are established, they are combined into a stage group. Here is what those groups generally indicate across skin cancers:
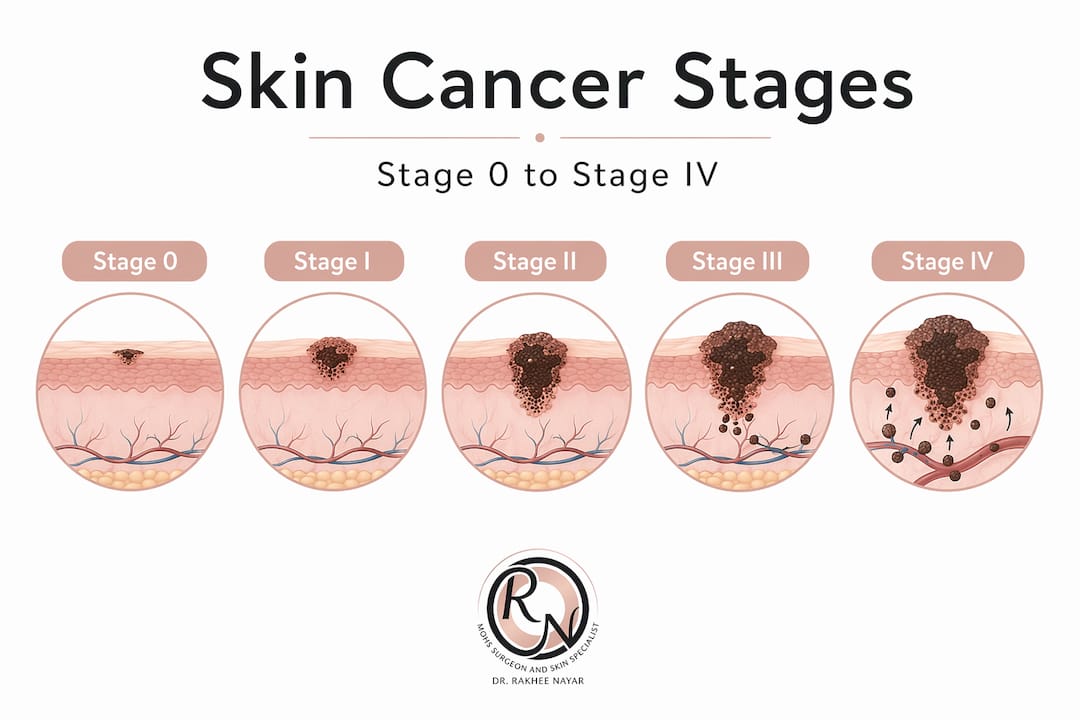
- Stage 0 (in situ): Cancer cells are present but confined entirely to the epidermis. No invasion has occurred. Treatment is usually straightforward excision with excellent outcomes.
- Stage I: A thin, localised tumour with no lymph node involvement. For melanoma this typically means Breslow depth under 2mm without ulceration. Surgery is usually curative, and survival rates correlate strongly with being caught at this stage.
- Stage II: A thicker or ulcerated localised tumour, still without nodal spread. Wider surgical margins are required and sentinel lymph node biopsy is standard for melanoma.
- Stage III: Cancer has reached the regional lymph nodes. Treatment expands to include lymph node surgery, adjuvant systemic therapies such as immunotherapy or targeted therapy, and sometimes radiation. This stage represents a meaningful shift in the treatment approach.
- Stage IV: Cancer has spread to distant sites. Prognosis is considerably more guarded. Stage IV disease requires aggressive treatment and may involve combinations of surgery, radiation, immunotherapy, and chemotherapy. For Merkel cell carcinoma, metastatic disease carries a five-year survival below 15%, underscoring how meaningfully stage affects prognosis.
The skin cancer prognosis based on stage is most favourable when the diagnosis occurs early. That is not a platitude. It reflects a measurable biological reality: early, shallow melanomas have a cure rate approaching 100% with surgery alone, whereas deeper tumours carry a significantly higher risk of metastasis. Knowing this reinforces why prompt investigation of suspicious changes matters. More guidance on what to look for is available in Mohssurgeon’s guide to skin cancer symptoms and early detection.
Staging: common misunderstandings
One of the most persistent misconceptions is that the stage of a skin cancer can be estimated from its appearance at a consultation. It cannot. Clinical examination alone cannot accurately stage skin cancer. A small, seemingly benign lesion may harbour deep microscopic invasion that places it in a higher stage, while a visually alarming mole may prove to be superficial and early.
Microscopic findings routinely change the staging and, by extension, the treatment plan. A melanoma that looked clinically like a stage I lesion may be reclassified after SLNB reveals microscopic lymph node involvement, shifting it immediately to stage III and triggering an entirely different treatment pathway.
Rare cancers like Merkel cell carcinoma add further nuance. Staging is not just a prognostic label for this cancer. It is the direct determinant of whether a patient receives radiation to regional lymph nodes or undergoes lymph node dissection in addition to wide local excision.
Finally, staging is never a solo decision. Accurate assessment requires a coordinated multidisciplinary team, typically including a dermatologist, pathologist, oncologist, and surgeon. The precision of that collaboration directly affects the accuracy of your stage assignment.
Pro Tip: If you receive a staging opinion without a biopsy result, ask why. Pathologic staging through tissue examination is the standard. Clinical staging alone is a starting point, not a final answer.
My perspective on staging and what it really means for patients
I have spoken with many people at the point where they have just received a staging result, and the emotional weight of that moment is real. Hearing “stage III” when you were hoping for “stage I” can feel devastating. What I have found, though, is that the stage is not a verdict. It is a map.
The patients who engage most effectively with their care are the ones who ask their surgeons what the stage means specifically for their tumour, not just the statistical average. Two people with a stage IIB melanoma may have very different clinical contexts, and treatment decisions should reflect that detail.
What I consistently tell people is this: understanding your stage is the most empowering thing you can do early in your treatment. It lets you ask sharper questions, understand why certain tests are ordered, and appreciate why one treatment is chosen over another. Staging is a tool that gives your medical team precision. Use that precision to your advantage.
Early detection genuinely matters here. The difference between a stage I and a stage III diagnosis can come down to months. If you have a suspicious lesion, getting it assessed promptly is not overreacting. It is the most rational thing you can do.
— Gregg
Precise staging, precise treatment at Mohssurgeon

When staging points to a skin cancer that needs careful, precise surgical removal, particularly on the face or cosmetically sensitive areas, the treatment approach matters as much as the diagnosis. Miss Rakhee Nayar at Mohssurgeon specialises in Mohs micrographic surgery, a technique that removes skin cancers layer by layer with immediate microscopic examination, achieving high cure rates while preserving as much healthy tissue as possible. This level of precision complements the detail that accurate staging provides. Whether you are newly diagnosed or seeking a second opinion, Mohssurgeon offers private consultations in North West England and e-consultations for patients across the UK and internationally. Explore the full range of skin cancer treatments available, and take the next step with a team that combines surgical expertise with genuine patient-centred care.
FAQ
What is skin cancer staging?
Skin cancer staging is the process of classifying how far a cancer has grown and whether it has spread, using the TNM classification system that accounts for tumour size, lymph node involvement, and distant metastasis.
Can a doctor stage skin cancer just by looking at it?
No. Visual examination alone cannot accurately determine stage. Biopsy and microscopic pathology are required, and sentinel lymph node biopsy is often needed to detect spread that imaging cannot reveal.
What stage is most treatable?
Stages 0 and I carry the best prognosis. Early, shallow melanomas have a cure rate approaching 100% after surgery, whereas deeper or metastatic disease requires more intensive treatment and carries a less favourable outlook.
Does staging differ between melanoma and other skin cancers?
Yes. Melanoma staging relies heavily on Breslow depth and ulceration status, while non-melanoma cancers like squamous cell carcinoma use tumour diameter, perineural invasion, and location. Merkel cell carcinoma staging directly determines treatment intensity and is not purely prognostic.
How long does skin cancer staging take?
The timeline varies. Initial biopsy results typically return within one to two weeks. Sentinel lymph node biopsy and imaging studies may add further time, but staging studies are tailored to your specific risk profile, so not every patient requires every test.


