
Basal cell carcinoma on the face, known clinically as facial BCC, is the most common form of skin cancer in the United Kingdom and arises predominantly on sun-exposed skin. Up to 80% of all BCCs occur on the face, a direct consequence of cumulative lifetime ultraviolet exposure. The cancer grows slowly but causes progressive tissue destruction if left untreated. Early recognition, accurate diagnosis, and specialist-led treatment are the factors that determine both cure rates and the quality of the final cosmetic result. This article explains what to look for, how facial BCC is diagnosed and treated, and what reconstruction involves.
What does BCC on the face look like?
Facial BCC presents in several distinct forms, and recognising the differences matters because each subtype carries a different level of aggressiveness. The most common presentation is a shiny, pearly nodule with small visible blood vessels on the surface, typically appearing on the nose, cheeks, or forehead. A second pattern is a persistent ulcer that bleeds, crusts, and refuses to heal over weeks or months. A third is a flat, scar-like area with an ill-defined edge, which is the morphoeic subtype and the most deceptive of all.
The sites most frequently affected on the face are the nose, eyelids, inner corners of the eye, temples, ears, and the skin around the mouth. These are precisely the areas that receive the highest cumulative sun exposure over a lifetime. BCC lesions can closely resemble benign conditions such as eczema, psoriasis, persistent pimples, or old scars, which is why many patients delay seeking advice for months or even years.
The ABCDE rule, widely used for melanoma, has limited direct application to BCC. Dermoscopy, a technique using a handheld magnifying device with polarised light, is far more useful. A trained clinician using dermoscopy can identify the arborising blood vessels, blue-grey ovoid nests, and leaf-like structures that characterise BCC subtypes with high accuracy.
- Nodular BCC: shiny, dome-shaped, pink or flesh-coloured bump with visible blood vessels
- Superficial BCC: flat, pink or red scaly patch, often mistaken for eczema or psoriasis
- Morphoeic BCC: pale, scar-like, firm plaque with poorly defined borders; the highest-risk subtype
- Pigmented BCC: contains brown or black pigment, occasionally mistaken for melanoma
Pro Tip: Any spot on your face that has not healed within four weeks, bleeds without injury, or looks like a scar where you have had no wound deserves a specialist opinion. Do not wait for it to change further.
How is facial BCC diagnosed and classified?
Diagnosis of facial BCC follows a structured pathway that begins with clinical examination and ends with histopathological confirmation. No treatment should proceed without a tissue diagnosis.
- Clinical examination: A specialist examines the lesion with the naked eye and dermoscopy, assessing size, borders, surface texture, and the presence of telangiectasia or pigmentation.
- Biopsy: A punch biopsy or shave biopsy is taken under local anaesthetic. The sample is sent to a histopathologist who confirms the diagnosis and identifies the subtype.
- Subtype classification: The histopathology report classifies the BCC as nodular, superficial, morphoeic, infiltrative, or basosquamous. This classification directly determines treatment choice.
- Risk stratification: Lesions are categorised as low risk or high risk based on size, site, subtype, and whether the tumour is primary or recurrent.
- Imaging: In rare aggressive cases, imaging should complement clinical assessment to determine tumour depth and guide surgical planning, particularly when bone involvement is suspected.
- Multidisciplinary team review: Complex or recurrent cases are discussed at a skin cancer multidisciplinary team meeting, involving dermatology, plastic surgery, oncology, and radiology.
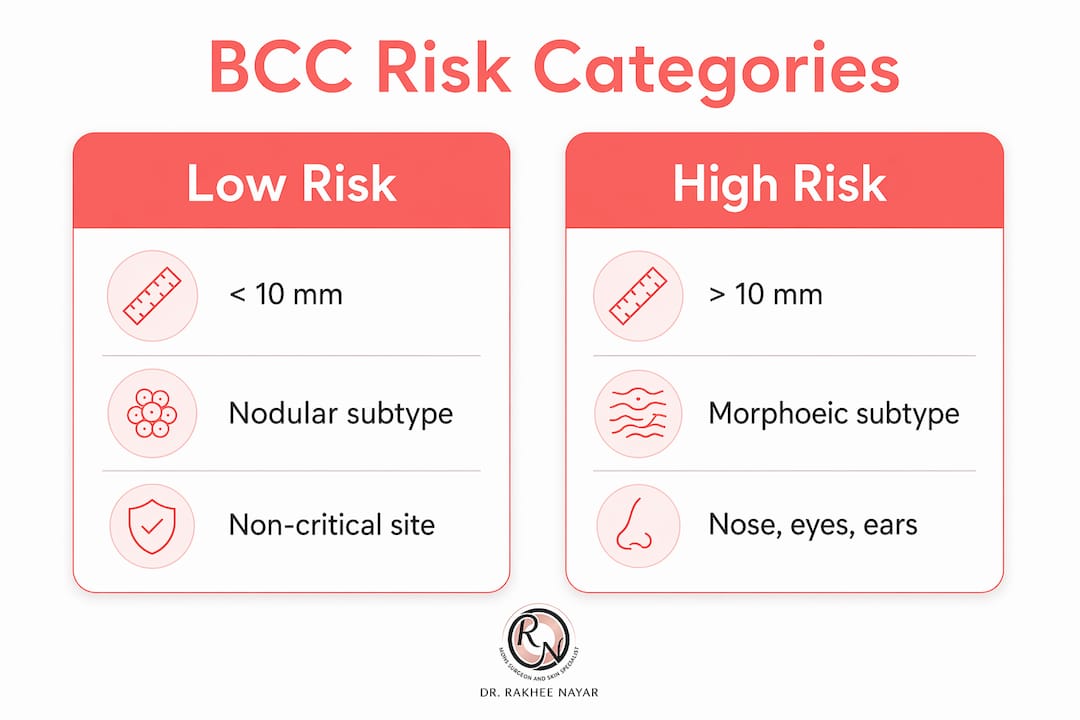
| Feature | Low risk | High risk |
|---|---|---|
| Size | Less than 10 mm on face | Greater than 10 mm on face |
| Subtype | Nodular, superficial | Morphoeic, infiltrative, basosquamous |
| Site | Cheek, forehead | Nose, eyelid, ear, temple |
| Borders | Well defined | Poorly defined |
| History | Primary lesion | Recurrent lesion |
Understanding your lesion’s risk category is not a formality. It determines whether standard surgical excision is appropriate or whether Mohs micrographic surgery is the recommended approach. For a detailed overview of identifying facial BCC, the clinical features that prompt referral are well documented.
What are the treatment options for BCC on the face?
Surgical excision and Mohs micrographic surgery are the two gold-standard treatments for facial BCC. The choice between them depends on the lesion’s subtype, size, site, and whether it is a primary or recurrent tumour.
Standard surgical excision
Standard excision removes the tumour with a margin of clinically normal skin, typically 3–5 mm for low-risk lesions. The excised tissue is sent for histopathology after the procedure. If the margins are not clear, a second operation is required. This approach is appropriate for well-defined, low-risk BCCs in sites where tissue conservation is less critical.

Mohs micrographic surgery
Mohs surgery is preferred for precise excision and reconstruction planning in cosmetically sensitive facial areas. The procedure involves removing the tumour in thin layers, with each layer examined under a microscope on the same day. Removal continues only in the direction where cancer cells remain. This means healthy tissue is preserved to the maximum extent possible, which is critical on the nose, eyelids, and ears where every millimetre of skin matters. Mohs micrographic surgery involves systematic margin assessment enabling maximal tissue conservation, which is the defining advantage over standard excision for high-risk facial sites.
| Treatment | Best suited to | Tissue preservation | Same-day margin check |
|---|---|---|---|
| Standard excision | Low-risk, well-defined BCC | Moderate | No |
| Mohs surgery | High-risk, recurrent, facial BCC | Maximum | Yes |
| Radiotherapy | Patients unfit for surgery | N/A | No |
| Vismodegib | Advanced or inoperable BCC | N/A | No |
Radiotherapy
Radiotherapy is an effective option for patients who are medically unfit for surgery or who decline an operation. It is also used as adjuvant treatment after surgery in cases with perineural invasion. The cosmetic result with radiotherapy tends to deteriorate over years, which is a relevant consideration for younger patients.
Hedgehog pathway inhibitors
Vismodegib is a targeted oral therapy that blocks the Hedgehog signalling pathway, which drives BCC growth. It is reserved for locally advanced or metastatic BCC where surgery is not feasible. In periocular BCC, vismodegib achieves a complete response rate of approximately 38% and a partial response in a further 39% of cases. However, recurrence after stopping therapy occurs in around 17% of patients, and adverse events including muscle cramps, hair loss, and fatigue are common. Medical therapies like vismodegib represent important alternatives for patients unsuitable for surgery, but require careful counselling regarding side effects and recurrence risk.
Pro Tip: If you are offered Mohs surgery for a BCC near your eye, nose, or ear, ask specifically whether your surgeon has dual training in both Mohs and plastic surgery. The two skills together produce the best functional and cosmetic result.
Early treatment prevents deep invasion and facial tissue destruction. In rare long-standing cases, bone invasion has been documented in large tumours on the nose and forehead, requiring complex craniofacial surgery. This outcome is avoidable with timely diagnosis and treatment.
How does facial reconstruction restore appearance after BCC removal?
Reconstruction after facial BCC excision is not cosmetic surgery in the elective sense. It is the restoration of normal anatomy, function, and appearance following cancer removal. The reconstructive plan is decided at the time of surgery, once the tumour has been fully cleared.
Facial reconstruction after BCC excision uses local flaps and skin grafts tailored to the defect’s size and location. Local flaps, where adjacent skin is repositioned to fill the wound, are preferred for smaller defects on the nose and cheeks because they match skin colour and texture closely. Skin grafts, taken from a donor site such as behind the ear or the upper eyelid, are used for larger defects on the forehead or temple where local tissue is insufficient.
- Local flaps: best for nasal tip, alar rim, and cheek defects; excellent colour match; heals in one stage
- Skin grafts: suited to larger or flat defects; may require two stages; slight colour difference initially
- Staged procedures: used when the defect is complex or when the surgeon wants to confirm clear margins before committing to reconstruction
- Eyelid reconstruction: requires specialist techniques to restore lid closure and protect the eye from corneal damage
- Nasal reconstruction: may involve cartilage grafts to maintain structural support alongside skin coverage
“The goal of reconstruction is not simply to close a wound. It is to restore the patient’s face as close to its pre-cancer state as possible, with full attention to function as well as appearance.” — Miss Rakhee Nayar
The psychosocial benefit of well-executed reconstruction is significant. Patients who achieve a good cosmetic outcome report higher confidence, reduced anxiety, and faster return to normal social activity. Realistic expectations are set before surgery: scars will be present but are designed to follow natural facial lines and fade over 12–18 months. Combining surgical precision with aesthetic expertise is the defining factor in optimising both cure and quality of life after facial BCC treatment.
Scar management after reconstruction includes silicone gel or sheeting from six weeks post-operatively, sun protection of the scar for at least 12 months, and massage once the wound is fully healed. In selected cases, laser treatment or steroid injections are used to refine the scar further.
What should patients know about monitoring and long-term care?
Treatment of facial BCC does not end at the operating table. Structured follow-up is a clinical requirement, not an optional extra.
- Follow-up schedule: Most patients are reviewed at three months, six months, and 12 months after treatment. High-risk cases or those treated for recurrent BCC are followed for five years.
- Recurrence recognition: 30% recurrence at five years has been reported in some series for high-risk lesions. Patients should know that a new shiny nodule, a non-healing area, or a change in the scar texture at the treatment site warrants urgent review.
- Self-examination: Monthly self-examination of the face in good light is recommended. Use a mirror to check the nose, ears, and hairline, which are easy to overlook.
- Sun protection: Daily broad-spectrum SPF 50 sunscreen on all exposed facial skin is the single most effective measure for preventing new BCCs. Protective clothing, hats with a brim, and avoiding midday sun between 11am and 3pm reduce cumulative UV damage further.
- New primary BCCs: Patients who have had one BCC have a significantly elevated risk of developing further primary BCCs elsewhere on the face or body. Annual skin checks with a specialist are advised for life.
- Lifelong dermatologic care: Patients with a history of multiple BCCs, immunosuppression, or Gorlin syndrome require more frequent surveillance and may benefit from chemoprevention strategies discussed with their specialist team.
Skin cancer prevention and recovery practices are well established and should form part of every patient’s long-term plan after facial BCC treatment.
Key takeaways
Facial BCC is highly treatable when caught early, but the choice of treatment and the quality of reconstruction determine both cure rates and long-term cosmetic outcomes.
| Point | Details |
|---|---|
| Early recognition matters | Up to 80% of BCCs occur on the face; any non-healing facial spot warrants specialist review. |
| Subtype drives treatment choice | Morphoeic and infiltrative BCCs require Mohs surgery; nodular BCCs may suit standard excision. |
| Mohs surgery preserves tissue | Same-day margin assessment removes only cancerous tissue, protecting healthy facial skin. |
| Reconstruction restores function | Local flaps and skin grafts are tailored to defect site to restore appearance and function. |
| Long-term follow-up is mandatory | Recurrence risk persists for years; annual skin checks and daily SPF 50 are lifelong requirements. |
What I have learned from treating facial BCC
By Miss Rakhee Nayar, Consultant Plastic Surgeon and Mohs Surgeon
The patients who do best are not necessarily those with the smallest tumours. They are the ones who were referred early, had a clear diagnosis before treatment began, and had reconstruction planned as part of the same surgical episode. What I see too often is a patient arriving after a BCC has been incompletely excised elsewhere, sometimes twice, with a scar that has obscured the tumour margins and made the Mohs procedure considerably more complex than it needed to be.
The nose is the site that demands the most respect. A 6 mm morphoeic BCC on the nasal ala can extend 15 mm or more beneath the surface. Standard excision with a 4 mm margin will not clear it. Mohs surgery will. The difference in tissue removed between the two approaches is the difference between a straightforward local flap and a forehead flap requiring two stages.
I also want to address the anxiety around reconstruction. Many patients assume that removing a BCC from the face will leave them disfigured. In the vast majority of cases, that is not the outcome. With careful planning, the scar sits in a natural crease or shadow line, and within a year most patients tell me they struggle to remember which side was treated. The key is having the reconstruction performed by someone who understands both the oncological and the aesthetic demands of the procedure simultaneously.
My advice to anyone reading this: do not delay a referral because you are worried about what treatment will involve. The earlier the referral, the simpler the surgery, and the better the result.
— Miss Rakhee Nayar
Expert Mohs surgery and facial reconstruction at Rakhee Nayar – Mohs Surgeon and Skin Specialist
If you have been diagnosed with or are concerned about a facial BCC, specialist assessment is the right next step.

Rakhee Nayar – Mohs Surgeon and Skin Specialist offers consultant-led Mohs surgery for facial BCC at Circle Cheshire, with Miss Nayar’s unique dual training in both Mohs and plastic surgery ensuring that tumour clearance and facial reconstruction are managed by a single expert. Private consultations and e-consultations are available for UK and international patients. For patients who want to understand their lesion before booking, the skin cancer symptoms guide provides a clear starting point. To discuss your diagnosis or arrange an assessment, contact the clinic directly.
This article is for information only and does not constitute medical advice. Consult a GMC-registered specialist for assessment and treatment of any skin lesion.
FAQ
What does BCC on the face look like?
Facial BCC most commonly appears as a shiny, pearly pink nodule with visible blood vessels, a persistent ulcer that does not heal, or a pale scar-like patch. BCC can closely resemble benign conditions such as eczema or old scars, which is why specialist assessment is needed.
Is Mohs surgery the best treatment for facial BCC?
Mohs micrographic surgery is the recommended treatment for high-risk facial BCCs, including those on the nose, eyelids, and ears, because it offers the highest cure rate while preserving the maximum amount of healthy tissue. Standard excision remains appropriate for low-risk, well-defined lesions in less critical facial sites.
Can facial BCC come back after treatment?
Yes. Recurrence is possible, particularly with morphoeic or infiltrative subtypes and in anatomically high-risk sites. Recurrence at five years has been reported in some series for high-risk lesions, which is why structured follow-up and annual skin checks are advised after treatment.
What reconstruction is available after facial BCC removal?
Reconstruction options include local skin flaps, skin grafts, and staged procedures, chosen according to the size and location of the defect. Eyelid and nasal reconstruction may also require cartilage grafts to restore structural support and function.
How can I reduce my risk of developing another BCC on my face?
Daily broad-spectrum SPF 50 sunscreen, protective clothing, and avoiding peak UV hours between 11am and 3pm are the most effective preventive measures. Patients with a history of facial BCC should have annual skin checks with a specialist for life, as the risk of further primary BCCs remains elevated.

