
TL;DR:
- Mohs surgery offers the highest cure rates for skin cancer, reaching up to 99% for primary basal cell carcinoma. Its precise, layer-by-layer technique examines 100% of tissue margins in real time, enabling complete tumour removal while sparing healthy tissue. Outcomes improve significantly when performed by fellowship-trained surgeons who combine surgical and pathological expertise.
When a doctor tells you that you need treatment for skin cancer, the first question most people ask is: “What are my chances?” The cure rates in Mohs surgery are among the highest of any skin cancer treatment available today, reaching up to 99% for primary basal cell carcinoma. Yet many patients either have not heard of Mohs micrographic surgery, or they carry misconceptions about what those numbers actually mean in practice. This article cuts through the confusion with evidence, comparisons, and clear explanations to help you make an informed decision about your care.
Key takeaways
| Point | Details |
|---|---|
| Exceptionally high cure rates | Mohs surgery achieves up to 99% for primary BCC, making it the most effective surgical option for skin cancer. |
| Recurrent cancer is also treatable | Even previously treated, recurrent skin cancers achieve 94 to 96% cure rates with Mohs surgery. |
| Full margin examination matters | Unlike standard excision, Mohs examines 100% of tissue margins in real time, directly explaining the superior outcomes. |
| Surgeon training shapes results | Fellowship-trained Mohs surgeons achieve the highest outcomes due to specialised microscopic pathology skills. |
| Comparison with other treatments | Radiation therapy achieves 90 to 95% cure rates for small cancers, notably lower than Mohs surgery’s figures. |
How Mohs surgery achieves such high cure rates
To understand the cure rates in Mohs surgery, you first need to understand what makes the procedure fundamentally different from a standard surgical excision or radiation therapy.
Mohs micrographic surgery is a precise, layer-by-layer technique performed under local anaesthetic. The surgeon removes a thin layer of tissue, maps it carefully, and then examines 100% of tissue margins under a microscope before removing the next layer. If cancer cells are still present at the edge of that layer, the surgeon removes another targeted sliver from only the affected area. This continues until the margins are completely clear.
Standard excision, by contrast, examines only a small fraction of the removed tissue under the microscope. Think of it like checking a handful of tiles on a roof rather than inspecting every single one. The vast majority of the margin never gets examined, which is why residual cancer cells can remain undetected. Mohs surgery closes that gap entirely.
Here is what the procedure typically involves at each stage:
- Tumour mapping: The surgeon draws a detailed map of the tissue specimen relative to its position on your skin.
- Layer removal: A thin horizontal layer of tissue is cut and processed on slides within the same appointment.
- Microscopic examination: Every edge, top, and bottom of that layer is examined under a microscope.
- Targeted re-excision: Only the areas where cancer cells remain are re-excised, preserving as much healthy tissue as possible.
- Wound closure: Once margins are clear, reconstruction or wound closure takes place, often on the same day.
This process is why Mohs surgery is particularly well-suited to cancers on the face, ears, nose, and eyelids, where tissue preservation matters enormously alongside cure.
Pro Tip: Ask any surgeon you consult whether they have completed a formal Mohs fellowship. Fellowship-trained surgeons perform both the surgical excision and the pathology review, which is the unique dual role that makes Mohs so effective.
Mohs surgery cure statistics by cancer type
The data on Mohs surgery outcomes is well established and consistent across multiple studies. Here is a clear picture of what the evidence actually shows.
For basal cell carcinoma (BCC), the most common form of skin cancer in the UK, Mohs cure rates reach 99% for primary (first-time) cases over a five-year follow-up period. Even for recurrent BCC, which is considerably harder to treat because previous surgery or radiation leaves scarred tissue that can hide tumour extensions, the five-year cure rate with Mohs is approximately 94.4%.
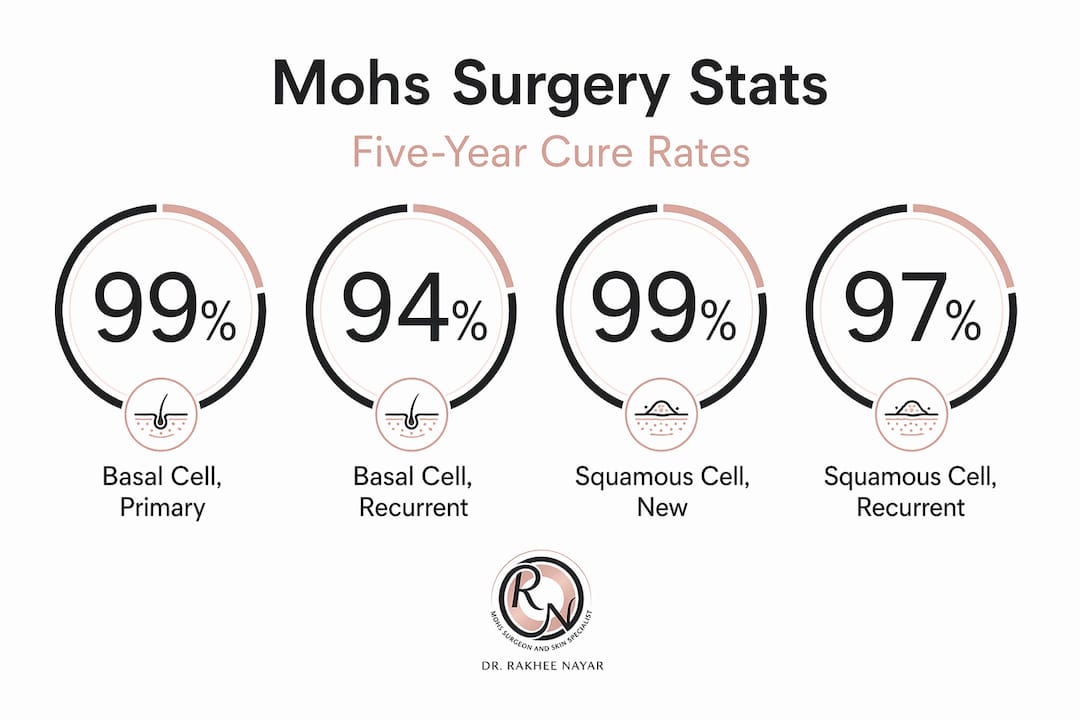
For squamous cell carcinoma (SCC), the second most common type, cure rates for new cancers exceed 99% and recurrent cases achieve approximately 94 to 96% cure rates. These figures are notably higher than what most alternative treatments can deliver.
| Cancer type | Status | Mohs cure rate (5-year) |
|---|---|---|
| Basal cell carcinoma | Primary (first occurrence) | Up to 99% |
| Basal cell carcinoma | Recurrent | Approx. 94.4% |
| Squamous cell carcinoma | Primary (first occurrence) | Over 99% |
| Squamous cell carcinoma | Recurrent | Approx. 94 to 96% |
What do these figures mean in practical terms? A 99% five-year cure rate means that for every 100 patients treated with Mohs for a new BCC, 99 will have no evidence of that cancer returning within five years. That is a genuinely remarkable outcome for a surgical procedure conducted under local anaesthetic in a single day.
It is worth noting that the phrase “cure rate” in oncology specifically refers to the absence of local recurrence within a defined follow-up period. Most studies use five years as the standard. It does not mean you are immune from developing a new, separate skin cancer in future, which is why lifelong skin surveillance remains important regardless of how successful your Mohs surgery is.
Comparing Mohs to other skin cancer treatments
When weighing up cancer removal with Mohs against other approaches, the numbers tell a clear story, but context matters too.
Mohs surgery achieves 98 to 99% for primary BCC, while superficial radiation therapy achieves 90 to 95% for small cancers. That gap may sound modest on paper, but in clinical reality it represents a meaningful difference in residual cancer risk, particularly for tumours in high-risk locations or with aggressive growth patterns.
| Treatment | Cure rate | Duration | Invasiveness | Suitable for |
|---|---|---|---|---|
| Mohs surgery | 98 to 99% (primary BCC) | Single day | Moderate (surgical) | Face, high-risk areas, recurrent tumours |
| Radiation therapy | 90 to 95% | 4 to 7 weeks | Low (non-surgical) | Patients unfit for surgery, low-risk tumours |
| Standard excision | 90 to 95% | Single day | Moderate (surgical) | Low-risk, straightforward tumours |
| Topical treatments | Variable (lower) | Weeks to months | Minimal | Superficial, low-risk BCC only |
Radiation therapy requires a 4 to 7 week treatment protocol, typically involving multiple sessions per week. For a patient who cannot tolerate surgery due to age or health conditions, it is a reasonable choice. However, for someone in good health with a tumour on the nose, eyelid, or ear, the combination of a single-day procedure and a significantly higher cure rate makes Mohs surgery the gold standard in most clinical guidelines.
Here are the scenarios where Mohs surgery typically offers the clearest advantage:
- Tumours in cosmetically sensitive or functionally critical areas (face, hands, genitals)
- Aggressive subtypes such as morphoeic or infiltrating BCC
- Recurrent tumours after prior treatment
- Large tumours or those with poorly defined borders
- Patients who want the highest possible certainty of complete removal
Pro Tip: If your tumour is on or near your face and you are otherwise well, ask specifically whether Mohs is appropriate for your case before accepting a referral for standard excision or radiotherapy. The cure rate difference is significant enough to justify the conversation.
Factors that influence Mohs surgery outcomes
Even within Mohs surgery, not every case carries identical odds. Several factors shape the final result, and understanding them helps you ask better questions during your consultation.
Surgeon expertise is arguably the most significant variable. Fellowship-trained surgeons produce the best outcomes because they perform both the surgical removal and the microscopic pathology assessment themselves. A surgeon without that dual training may have to rely on external pathology reporting, which introduces delays and reduces the real-time precision that defines the technique.

Tumour characteristics also play a major role. Superficial BCCs on the back or chest carry a very different risk profile from morphoeic BCCs at the inner corner of the eye. Size, depth, subtype, and whether the tumour has been treated before all affect how complex the case will be and, consequently, how many surgical stages are required.
Other key patient considerations include:
- Location: Tumours on the face, ears, and lips benefit most from Mohs surgery because tissue preservation is critical alongside achieving clear margins.
- Recurrence history: Previously treated tumours develop in scar tissue, making standard margin assessment less reliable and Mohs even more valuable.
- Tumour subtype: Aggressive histological subtypes have a higher risk of subclinical extension, meaning the visible tumour underestimates the true size. Mohs surgery handles this more reliably than other methods.
- Patient health and preferences: While Mohs is highly effective, suitability also depends on your overall health, ability to tolerate local anaesthetic, and access to a trained specialist.
Separating Mohs surgery myths from facts is also worthwhile. One common misconception is that a high cure rate means recurrence is impossible. Another is that Mohs is only for severe cases. In truth, it is appropriate for a wide range of BCC and SCC presentations, particularly those in anatomically sensitive locations.
Recovery, monitoring, and what to expect
Knowing the cure statistics is only part of the picture. Understanding the procedural experience and what follows is equally important for setting realistic expectations.
A typical Mohs surgery day unfolds like this:
- Arrival and preparation: The area is cleaned and local anaesthetic administered. You remain awake throughout.
- First excision: The visible tumour and a thin surrounding margin are removed.
- Processing and waiting: The tissue is processed and examined under a microscope. This takes approximately 45 to 60 minutes per stage.
- Further stages if needed: If cancer cells remain, the process repeats. Most cases require one to three stages.
- Wound closure: Once clear margins are confirmed, the wound is closed, often with a repair or flap, and you are discharged the same day.
Recovery typically involves some swelling, bruising, and wound care for two to four weeks. Most patients return to normal activities within a few days. Wound healing varies depending on location and repair method, but the majority of patients report satisfactory cosmetic outcomes.
Monitoring for skin cancer recurrence after surgery involves regular skin checks with your specialist. Most clinicians recommend three to six monthly reviews for the first two years, then annual checks thereafter. Early detection of any new lesion significantly improves the success of secondary treatment.
My perspective on what these numbers actually mean
I have spent years writing about medical decision-making, and the question that always sits beneath the statistics is this: what does a 99% cure rate feel like when you are the patient sitting in front of the consultant?
In my experience covering surgical outcomes and patient communication, the most significant challenge is not the numbers themselves. It is the misunderstanding of what those numbers represent. Patients often hear “99% cure rate” and assume that means a 1% chance of dying from skin cancer. It does not. It refers to local recurrence at the treated site within five years. That distinction matters enormously for how patients process the decision and how much anxiety they carry into surgery.
What I find most compelling about Mohs surgery outcomes is that the high cure rates are not a marketing claim. They come directly from the technical mechanism of the procedure: examining 100% of the margin in real time rather than sampling. That is not a claim about surgeon skill or clinic prestige. It is a structural advantage built into the method itself.
The other point I would press firmly is this: where you go for care genuinely changes your odds. A fellowship-trained surgeon who understands both the surgery and the pathology is not interchangeable with someone who does occasional excisions. The data on surgeon expertise confirms this consistently, and it is the kind of detail that gets lost when patients focus solely on cost or convenience.
If you are weighing up your options after a diagnosis, the cure statistics should give you real confidence that Mohs surgery, done by the right specialist, is the most evidence-supported choice available for the cancers it treats.
— Gregg
Expert Mohs surgery care at Mohssurgeon

If you are considering Mohs surgery after a diagnosis or want a specialist opinion on a suspicious lesion, Mohssurgeon offers expert micrographic surgery led by Miss Rakhee Nayar, who holds dual training in both plastic surgery and Mohs surgery. That combination is rare and directly relevant to achieving the highest possible cure rates while preserving cosmetic outcomes. Whether you are seeking a first consultation, a second opinion, or guidance on skin cancer detection, the clinic provides in-person and e-consultations for UK and international patients. You can also explore detailed information on the Mohs surgery procedure and what to expect at every stage of your treatment.
FAQ
What is the cure rate in Mohs surgery for basal cell carcinoma?
Mohs surgery achieves a five-year cure rate of up to 99% for primary basal cell carcinoma and approximately 94.4% for recurrent cases, making it the most effective treatment option currently available.
How do Mohs surgery cure statistics compare to radiation therapy?
Mohs surgery achieves 98 to 99% cure rates for primary BCC, compared to 90 to 95% for superficial radiation therapy, which also requires a treatment protocol lasting four to seven weeks.
Does a high cure rate mean the cancer cannot come back?
Not exactly. The cure rate refers to the absence of local recurrence at the treated site within five years. You can still develop new skin cancers elsewhere, which is why regular skin surveillance after Mohs surgery remains important.
How does surgeon training affect Mohs surgery outcomes?
Fellowship-trained Mohs surgeons perform both the surgical excision and the microscopic margin assessment themselves, which is the dual role directly responsible for the procedure’s superior cure rates compared to standard excision.
Is Mohs surgery suitable for squamous cell carcinoma as well as BCC?
Yes. Mohs surgery achieves over 99% cure rates for primary squamous cell carcinoma and approximately 94 to 96% for recurrent cases, with outcomes comparable to those seen in basal cell carcinoma treatment.


