
A multidisciplinary team (MDT) in skin cancer is a coordinated group of specialists who collectively develop an individualised treatment plan for each patient. The role of multidisciplinary team in skin cancer management is defined by NICE guidance and British Association of Dermatologists (BAD) standards as the clinical standard of care for all confirmed or suspected skin cancers. At Rakhee Nayar – Mohs Surgeon and Skin Specialist, this collaborative model underpins every complex case, ensuring that decisions on surgery, systemic therapy, and reconstruction draw on the full breadth of relevant expertise. The result is a treatment plan shaped by tumour biology, patient health, and the best available evidence, rather than the view of any single clinician.
What specialists make up the skin cancer multidisciplinary team?
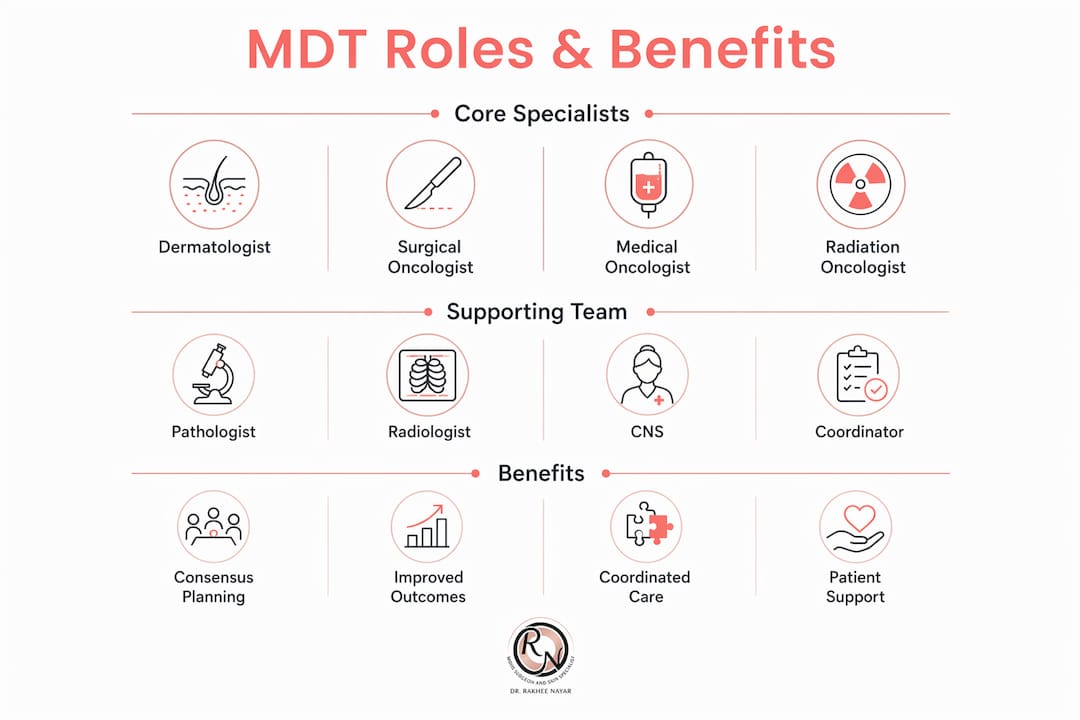
The skin cancer treatment team in the UK typically brings together dermatologists, surgical oncologists, medical oncologists, radiation oncologists, pathologists, and radiologists. Each specialist contributes a distinct layer of clinical knowledge that no single discipline can replicate alone.
Dermatologist. The dermatologist leads initial assessment, dermoscopy, and biopsy. They identify lesion characteristics and refer appropriately to the wider team.
Surgical oncologist or Mohs surgeon. This specialist plans and performs surgical excision, including Mohs micrographic surgery for high-risk or cosmetically sensitive tumours. Miss Rakhee Nayar holds dual training in plastic surgery and Mohs surgery, which means she can address both tumour clearance and reconstruction within the same consultation.
Medical oncologist. The medical oncologist manages systemic treatments, including immunotherapy agents such as cemiplimab for advanced squamous cell carcinoma (SCC). Their input is particularly important when surgery is not the primary option.
Radiation oncologist. Radiotherapy may be recommended as a primary treatment or as an adjunct after surgery for high-risk cases. The radiation oncologist advises on dose, field, and fractionation.
Pathologist. The pathologist provides the definitive tissue diagnosis. Their histology report, including tumour subtype, margins, and perineural invasion, directly shapes the MDT’s treatment recommendation.
Radiologist. Imaging review by the radiologist clarifies tumour extent, nodal involvement, and distant spread. This is especially relevant for melanoma and high-risk non-melanoma skin cancers.
Clinical nurse specialist (CNS). The CNS is the patient’s primary point of contact throughout the care pathway. They translate MDT decisions into plain language, coordinate appointments, and provide emotional support.
MDT coordinator. The coordinator manages administrative functions: scheduling meetings, maintaining records, and communicating treatment plans to the wider clinical team after each MDT discussion.
Pro Tip: When attending your first consultation after a skin cancer diagnosis, ask specifically whether your case will be discussed at an MDT meeting. Knowing this happens gives you confidence that your plan reflects expert consensus, not a single opinion.
How does the MDT meeting process work in skin cancer care?
NHS MDT meetings for skin cancer typically take place weekly. The format is structured and time-limited, with cases reviewed in sequence by the assembled specialists.
The process follows a consistent pattern:
- Case pre-screening. Before the meeting, the MDT coordinator and lead clinician identify which cases require full MDT discussion. Straightforward low-risk cases may be managed without a full panel review, preserving specialist time for complex presentations.
- Clinical data review. The team reviews histology reports from the pathologist, imaging from the radiologist, and relevant patient health data. This background review happens before the meeting begins, so discussion focuses on interpretation and decision-making rather than data gathering.
- Consensus discussion. Specialists debate treatment options based on tumour stage, location, molecular profile, and patient fitness. The discussion may cover surgery, radiotherapy, systemic therapy, or a combination.
- Treatment recommendation. The team reaches a consensus recommendation. This is documented formally and communicated to the referring clinician and the patient’s CNS.
- Patient communication. The CNS contacts the patient after the meeting to explain the recommendation, answer questions, and arrange next steps. Patients do not attend MDT meetings themselves.
Pro Tip: If you are a healthcare professional referring a case, submit a clear summary of the patient’s comorbidities, current medications, and performance status alongside the histology. Incomplete referrals slow consensus and can delay treatment.
Understanding how skin cancer mapping informs this process helps clarify why detailed pre-operative data matters so much to the MDT’s final recommendation.
What are the benefits of a multidisciplinary approach in managing skin cancer?
The multidisciplinary approach in cancer care produces measurably better outcomes for patients with skin cancer, particularly those with complex or advanced disease. The core benefit is that no single specialist’s blind spot determines the treatment plan.
Key clinical benefits include:
- Broader treatment options. The MDT can identify patients who are not surgical candidates and route them towards systemic therapy. In one case series of 130 patients, 37.9% of SCC cases were candidates for cemiplimab rather than primary surgery. That figure shows how often surgery alone would have been an incomplete answer.
- Reduced treatment variation. Collective decision-making reduces the risk that a patient’s outcome depends on which individual clinician they happen to see first.
- Integration of systemic therapies. Medical oncologists within the MDT ensure that immunotherapy and targeted agents are considered alongside surgical and radiation options, particularly for high-risk skin cancer presentations.
- Improved patient education. CNS involvement means patients receive consistent, accurate information about their diagnosis and treatment options, which supports shared decision-making.
- Coordinated follow-up. The MDT agrees on surveillance intervals and recurrence monitoring, reducing gaps in post-treatment care.
The table below summarises how each MDT benefit translates into a direct patient outcome.
| MDT benefit | Patient outcome |
|---|---|
| Consensus treatment planning | Reduced risk of under- or over-treatment |
| Systemic therapy identification | Access to immunotherapy for inoperable SCC |
| CNS patient liaison | Better understanding of treatment and reduced anxiety |
| Radiologist input on staging | Accurate nodal and metastatic assessment |
| Coordinated follow-up plan | Earlier detection of recurrence |
The importance of teamwork in oncology is most visible in cases where a single-specialty approach would have missed a critical factor. A patient with SCC and perineural invasion, for example, requires input from the pathologist, radiation oncologist, and surgeon simultaneously. No one specialist holds all three perspectives.
What challenges affect the effectiveness of skin cancer MDTs?
Skin cancer incidence is rising in the UK, and that volume places real pressure on MDT capacity. The challenges are structural, not a reflection of individual clinician effort.
- Meeting time pressure. As referral numbers grow, weekly MDT slots fill quickly. Without pre-screening protocols, complex cases compete for discussion time with straightforward ones, reducing the quality of debate for both.
- Staffing gaps. Full MDT function requires all core specialties to be represented. Vacancies in pathology or radiology can delay case review or force decisions without complete data.
- Technology for virtual meetings. Virtual and hybrid MDT meetings are increasingly used to include remote specialists, but they require reliable platforms and clear protocols to avoid wasted clinical time.
- Communication between disciplines. Terminology and priorities differ between specialties. A pathologist’s description of “close margins” may carry different weight for a surgeon than for a radiation oncologist. Structured reporting templates reduce this ambiguity.
- Patient communication delays. When MDT recommendations are not communicated promptly to patients, anxiety increases and treatment start times lengthen.
Efficient MDT workflow relies on case pre-screening protocols that focus specialist discussion on complex or outlier cases. This is not a shortcut. It is the mechanism that protects the quality of discussion for the patients who need it most.
How can patients engage with and benefit from the MDT approach?
Patients do not attend MDT meetings, but they are central to the process. The MDT’s recommendation is built around the individual patient’s tumour, health status, and personal circumstances.
Here is what patients can expect and do:
- Expect to be informed, not present. Your CNS will contact you after the MDT meeting to explain what was discussed and what the team recommends. This is standard practice across NHS and private settings.
- Ask your CNS specific questions. The CNS is your main contact. Ask them which specialists reviewed your case, what treatment options were considered, and why the recommended plan was chosen over alternatives.
- Understand your treatment plan in writing. Request a written summary of the MDT recommendation. This helps you recall details and share information with your GP or other treating clinicians.
- Engage in shared decision-making. The MDT recommendation is a clinical consensus, not a fixed instruction. You have the right to discuss alternatives, ask about clinical trials, and factor your own priorities into the final decision.
- Prepare for your consultation. Write down your questions before appointments. Bring a list of current medications and any relevant medical history that your team may not yet have.
The role of patient education in skin cancer outcomes is well established. Patients who understand their diagnosis and treatment plan are better placed to adhere to follow-up schedules and report new symptoms promptly.
Pro Tip: Before your first post-MDT consultation, write down three questions: What is the goal of my treatment? What are the risks of the recommended option? What happens if I choose not to proceed? These three questions cover the clinical essentials and give your CNS a clear structure to work through with you.
The skin cancer nurse specialist plays a critical liaison role, making the MDT’s clinical decisions understandable and accessible to patients. This function is what converts a clinical consensus into a care pathway the patient can actually follow.
Key takeaways
The role of multidisciplinary team in skin cancer is to produce a consensus treatment plan that no single specialist could generate alone, reducing variation and improving outcomes for every patient.
| Point | Details |
|---|---|
| MDT composition | Six core specialties plus CNS and coordinator form the standard UK skin cancer team. |
| Weekly meeting structure | NHS and private MDTs meet weekly to review histology, imaging, and patient data. |
| Systemic therapy access | MDT review identifies patients suited to immunotherapy rather than surgery alone. |
| CNS liaison role | The clinical nurse specialist translates MDT decisions into patient-facing guidance. |
| Patient engagement | Patients do not attend meetings but should ask their CNS for a written summary of recommendations. |
Why MDTs matter more than most patients realise
Patients often assume that their treatment plan comes from the surgeon or dermatologist they see in clinic. In reality, for any confirmed or high-risk skin cancer, that plan has been shaped by a room full of specialists who never met the patient directly. I find that this surprises people, and it should not.
In my practice, the MDT is where the genuinely difficult cases get resolved. A patient with a large SCC on the temple, perineural invasion on histology, and a history of immunosuppression cannot be managed by surgery alone. The radiation oncologist, the medical oncologist, and I need to agree on sequencing before a single incision is made. That conversation, conducted with full pathology and imaging in front of us, produces a plan that is categorically better than any one of us could have produced independently.
What I have observed over years of practice is that the MDT’s value is not evenly distributed. For straightforward basal cell carcinomas, the team confirms what the treating clinician already knew. For complex cases, the MDT is the difference between an adequate plan and the right plan. The challenge is that patients rarely know which category they fall into until the MDT has met.
Virtual MDTs are changing the model. Including a specialist from another centre via video adds expertise without requiring travel. The technology works when the protocols are clear. When they are not, the meeting loses focus and the benefit disappears. I would encourage any patient to ask their team whether their case was discussed in a full MDT, and if so, who was in the room.
— Miss Rakhee Nayar
Expert skin cancer care with MDT-informed treatment planning
Rakhee Nayar – Mohs Surgeon and Skin Specialist offers consultant-led skin cancer care that integrates MDT decision-making with specialist Mohs surgery and facial reconstruction. Miss Nayar’s dual training in plastic surgery and Mohs surgery means that surgical planning and reconstructive outcomes are considered together from the outset, not as separate steps.

Private consultations are available at Circle Cheshire in North West England, with e-consultations for patients across the UK and internationally. For patients with confirmed or suspected skin cancer, an early consultation allows Miss Nayar to assess whether MDT review is indicated and to coordinate referrals where needed. Learn more about Mohs micrographic surgery and how it fits within a broader MDT-led treatment plan, or review the full range of skin cancer services available through the practice.
This article is for informational purposes only and does not constitute medical advice. Consult a GMC-registered specialist for assessment and treatment recommendations specific to your situation.
FAQ
What is a multidisciplinary team in skin cancer?
A skin cancer MDT is a group of specialists, including dermatologists, surgeons, oncologists, pathologists, radiologists, and clinical nurse specialists, who meet regularly to agree on treatment plans for individual patients. Their collective input ensures that all relevant clinical factors are considered before treatment begins.
Do patients attend MDT meetings?
Patients do not attend MDT meetings. The team reviews histology, imaging, and clinical data independently, then communicates the agreed recommendation to the patient through their clinical nurse specialist.
How does a multidisciplinary team improve outcomes in skin cancer?
MDT review reduces treatment variation, identifies patients suited to systemic therapies rather than surgery, and coordinates follow-up care. Research shows that 37.9% of SCC patients in one case series qualified for immunotherapy rather than primary surgery, a finding that requires MDT input to act on safely.
What role does the clinical nurse specialist play in the MDT?
The clinical nurse specialist acts as the patient’s main contact, explaining MDT recommendations in plain language, coordinating appointments, and supporting shared decision-making throughout the treatment pathway.
How often does a skin cancer MDT meet?
Skin cancer MDTs in NHS and private practice typically meet weekly, reviewing new referrals and ongoing cases to maintain timely decision-making aligned with clinical need.


